The ravages of mental illness continue to flood every corner of society. Coverage of this atrocity has improved in quantity and sophistication in the last quarter-century–but to what end? Policy-makers, law enforcement and public opinion remain largely indifferent to meaningful education and reform. Mis-diagnoses, non-diagnoses, incarceration, hospital indifference, and violent deaths of people in psychosis surge on, gathering speed. And no one is at the wheel.
This strongly observed and written story by Hannah Dreier of TheWashington Post throws light into an especially neglected precinct: Poor black families, and the mentally afflicted children within those families. It provides a glimpse of the day-to-day crises of a divorced Black mother, Kelli, and her two sons–one of whom, the 11-year-old Ahav, is diagnosed with schizophrenia.
You may read Dreier’s piece as simply a searing journey into the wilderness of one family’s mental-illness misery, and of the heroic efforts of Kelli to keep Ahav safe. A closer reading reveals a miasma of bureaucratic obstacles, therapeutic failure, option-choking poverty, and the constant dread of trigger-happy law enforcement that imprison tens of thousands of families such as Kelli’s in the rusted chains of our failed mental healthcare system.
In the 1960s the breakaway Scottish mystic/psychiatrist R. D. Laing was prominent among many emerging voices proclaiming that mental illness does not exist. His aphorisms such as “Insanity [is] a perfectly rational adjustment to an insane world” and “Madness need not be all breakdown. It may also be break-through . . . ” made him a charismatic figure among the counter-culture. His work placed him in the company of the greatest denier of them all, Thomas Szasz, whose 1961 book, The Myth of Mental Illness, crippled the status of psychiatry for generations.
In that time, neuroscientists and psychiatrists worked patiently to rebuild the legitimate acceptance of mental illness and its destructive properties. Breakthrough advances in microcomputer technology established, for instance, that schizophrenia is a genuine disease of the human brain, and not just a synonym for “nut job”: it leaves lesions–tiny traces–in the brain; its clusters of flawed genes are genetically inherited and, to date, incurable.
Yet even as science (that fake mumbo-jumbo!) has steadily clarified the properties of mental illness at the top levels of discourse on the subject, its work is being rapidly undermined again where it counts: in the chaotic maw of popular culture, where malign ideology, semi-literacy, and poisonous cynicism threaten to nullify reason. Including reasoning about unreason.
Thus when the ineffable birdbrain Ann Coulter tweet-tweets, as she did on August 27, that she wants the deranged teenaged lethal shooter Kyle Rittenhouse to be her president (above), we may think of her as the hideous drum majorette at the head of a long malign parade, marching directly toward a new Dark Age.
. . . And perhaps more than a year before reviews of the Linden Cameron shooting by Salt Lake City police are completed. (Linden, a 13-year-old victim of Asperger’s syndrome, absorbed eleven bullets from a policeman’s service pistol on the night of Sept. 4, yet survived and remains in serious condition.)
Linden Cameron
The link below, to the latest update on Linden’s story, discusses this likelihood. The story was reported and written by Heidi Hatch and Mackenzie Ryan of KJZZ television in Salt Lake City.
Mundane reasons. Case backlogs. Scant resources to investigate them. That sort of thing. Since January of 2011, the Salt Lake City area has seen one hundred four shootings by police. Of these, only eight have been ruled “unjustified”–a fair microcosm of the national picture. Charges were filed in just three of the eight “unjustified” shootings, Hatch and Ryan report.
All three of those cases were dismissed.
Nine other unreviewed cases are piled on top of Linden Cameron’s.
And so Linden and his mother Golda Barton will wait. And wait. And wait. The state of waiting and its attendant stress, for one bureaucratic reason or another, is familiar to thousands of families trying to safeguard a mentally ill loved one, or to seek justice for that victim.
Below my September 22 blog on Linden’s case, a reader posted: “I will wait to see all the evidence.” I respect this reader’s sense of fairness. Yet we may never “see all the evidence.” That blog included a murky 36-second excerpt of body-cam recording released by the Salt Lake City police department. It shows a wandering pool of harsh light (presumably the camera light) surrounded by darkness. Linden can be glimpsed walking away from the camera before he disappears into the dark. We hear gunshots when the pool of light finds him again, he is writhing on the sidewalk. Then he turns over onto his left side and stops moving. We can hear him say,
“I don’t feel good. Tell Mom I love her.”
The body-cam footage below apparently covers the full length of the police video. It lasts 1 minute 40 seconds, some of the extra length showing police leaving their patrol car and yelling at Linden before the gunfire. It was posted on YouTube by the website RAW.
This footage also shows that Linden broke into a run after walking a few paces. The police pursue him in a 45-second footrace, yelling for him to “Get on the ground.” Then the shots and the boy’s moaning voice as he lies wounded on the sidewalk.
And that’s about it.
So: Linden Cameron and his mother, not to mention the police officers involved, probably will have to wait for up to a year, and maybe longer, before the investigative bureaucracy gets around to this case.
The great 19th-century British prime minister William Gladstone is credited with the maxim, “Justice delayed is justice denied.” Gladstone should have stuck around.
In a year’s time, pending investigations often lose their initial urgency. Public opinion and news coverage dissipate. The indignation of civic leaders cools. The cop shooting of a mentally ill boy, which initially drew international attention, grows stale in the files. The investigative bodies–in this case, they include an outside police department and the Salt Lake City department as well–tend to lose whatever incentive they may have had to render judgment against their own. The Linden Cameron case becomes something of an abstraction. Besides, it was dark. The camera dances around. Who, really, can say what happened? (Who, really, by this time, cares?)
“I will wait to see all the evidence.” A reasonable and honorable suspension of judgment.
I almost wrote, “the mentally ill people of America lost a hero on Sunday,” but that would not have been nearly adequate to contain this giant’s significance to our country.
Dj Jaffe, who succumbed to leukemia and other cancers at age 65 after stoically battling them for fifteen years, was a human beacon of hope and guidance and enlightenment to those who suffered from chronic brain diseases (“chronic” meaning genetically inherited and incurable). And to their caretaking relatives, mostly mothers, in practice; to their often overmatched doctors and therapists; to uninformed policymakers and corrections officers.
Pete Early
E. Fuller Torrey
Dj was among the three most influential advocates for the mentally ill in the brief history of that calling, along with the author and blogger Pete Earley and the pioneering statesman of advocacy, E. Fuller Torrey, author of many books and the founder of the Treatment Advocacy Center. The TAC website is the largest, most diverse compendium of m.i. information online.
Dj Jaffe was a skinny force of nature the likes of which the cautious mental healthcare world had never seen, and not everyone liked him. He walked away from an obscure career in advertising after the sister of his wife, Rose, was stricken with mental illness thirty years ago. Razor-sharp and pugnacious when he had to be, he transformed himself into an expert on the nosology, neuroscience, politics and policy issues surrounding the disease. Wearing his unrepentant bluejeans, ponytail, and oversize glasses (and a wrinkled suit when he had to), Dj mastered libraries of information, then cycloned through public hearings, press interviews, and panel discussions, rising to challenge the dignitaries who did not know what they were talking about—or didn’t care. He delighted in getting thrown out of hearings. Opponents were infuriated by his refusal to back down from a stance or a demand. Truth to tell, he was not always right.
He was right often enough. Boring in on our slipshod structure of criminal justice for the insane, he was instrumental in pushing the act known as Kendra’s Law, which allows courts to order treatment for certain mentally ill and perhaps dangerous patients even if they resist it. He worked with the Pennsylvania Republican congressman Tim Murphy to achieve the Helping Families in Mental Health Crisis Act. He demanded, and largely achieved, a long-delayed recognition that “chronic mental illness”—genetically inherited and incurable brain afflictions such as schizophrenia and bipolar disorder—differs on a quantum level from such lesser complaints as depression, alienation, alcoholism, and drug abuse.
In 2017 Pete Earley distilled the reasons why this distinction is essential:
“The problem, according to Jaffe, is that the focus, money and attention in our nation is focused on helping nearly everyone but those ten million [with chronic m.i.] and the result is at least 140,000 SMI Americans being homeless, 392,037 in jails and prisons, 755,360 on probation or parole and at least 95,000 who need hospitalization unable to find a bed.”
His politics were less doctrinaire than fluid, tuned to the needs of the dispossessed who consumed his passions. He founded the nonpartisan Mental Illness Policy Organization. As an adjunct fellow at the conservative Manhattan Institute, Dj spoke at a White House summit on mental illness in December 2019. His countless articles and appearances across the media spectrum testify that he was a zealot not for ideology, but for enlightenment and hope.
Dj joined Fuller Torrey and TAC in 1998. He drew on Torrey’s collaborative expertise and on TAC’s informational and advocacy riches for his important 2017 book, Insane Consequences: How the Mental Health Industry Fails the Mentally Ill (Prometheus Books).Torrey acknowledged his friend and disciple’s stature in a statement released this morning:
“Since 1998, when we first started making plans for what became the Treatment Advocacy Center, Dj has been the single most effective advocate I have worked with and a close personal friend. His dedication to improving the treatment of people with serious mental illness, based on his experience with his sister-in-law, has been extraordinary. The amount of time and energy he has invested in this mission, first at TAC and then at Mental Illness Policy Org, is legendary. Even as he knew he was dying, DJ said nothing and continued his advocacy efforts.”
On a personal note:
It took me a while to get comfortable with the idea of meeting Dj Jaffe. His reputation as a controversial know-it-all firebrand put me off. But when we did meet, the rapport was instant. We discovered that we could make one another laugh. (I nearly lost it in a hotel coffee house in New York when my friend got embroiled in an argument with the waiter. This was no ordinary waiter-customer spat: the waiter was yelling at Dj!) Over several breakfasts, dinners and drinks in New York, Washington, and in the Powers home in Vermont, and in many lively emails, we kept up a bantering style that could segue seamlessly into explorations of our passions and ideas.
His just-beneath-the-surface humor proved the key to Dj: The firebrand was a necessary tactic, not a character flaw. In fact, Dj Jaffe was an extraordinarily loving man, as his career shift after his sister-in-law’s illness demonstrates. He enjoyed a longstanding marriage to his wife Rose, a lovely, laughing woman whom he adored. When Rose died two years ago, his friends expected that Dj would be devastated with grief. He may have been, but he was back to his advocacy work in a day or two. He never mentioned his feelings.
He met a woman named Paula about a year and a half ago, via a dating app. She was the one who reached out to him, friends say. Dj probably knew at the time that he was dying. Paula and Dj were married on Friday in his hospital room. Paula wore white pajamas and stomped on a Styrofoam cup. By all accounts, the marriage was a happy one. Because that’s the kind of guy Dj Jaffe was.
The voices of the growing grass-roots movement to reform mental healthcare are at last rallying to demand justice for perhaps the most dispossessed victim in America.
In a town in America, here in the Twenty-first century, a man has been left to die. A maimed and blind and deeply mentally ill man.
He has been left to die in this town for thirteen years. Right out in public, on the city streets, where everybody can see him. And beat him and rob him when they feel like it. And nobody with any statutory power over his predicament seems to give a damn.
A technical clarification: this man is not on the streets of Vacaville as I write these words. He is in critical condition in a hospital, bandaged and splinted and broken after being struck by a car at a traffic intersection at dusk on February 12. (It is the second time this man has been hit.)
His injuries include a fractured skull and bleeding from the brain, facial lacerations, lung contusions, a dislocated shoulder, a shattered elbow, a decimated leg, and bruises that blanket his body.
Mark Rippee
But it’s a safe bet that after the surgeons have him all fixed up—it could take months—he will be ushered back out onto the streets, where the cars he can’t see and the thugs whom he cannot fend off will help him resume his accustomed existence.
The man has a name: (James) Mark Rippee. The city has a name: Vacaville, California. The situation has a name: depraved indifference to the survival of a human being.
I just made that name up. Actually, I borrowed it from legal parlance. Its definition: “Conduct which is so reckless, wanton and deficient and lacking in regard for the lives of others as to warrant the same culpability as the individual who actually commits a crime.”
Here is the crime that Mark Rippee has committed: the crime of existing while crippled, blind, and insane. Are there any questions?
I’m sure there are lots of questions. I have lots of questions myself. Or I used to. I have written so often about Mark Rippee since I became aware of his plight that the words I write about him seem to turn to dust. I have written blog posts about him here and here and here. I have written speeches to mental-health reform groups in which I summarize his story. I have written directly to media outlets, to lawmakers, and to civic leaders in Vacaville and elsewhere. And the streets still claim Mark Rippee.
The bare-bones story—as it were—is that Mark Rippee was involved in a terrible motorcycle crash in June 1987, at age 24, that left him nearly dead, with bits of his brain scattered near the site, his eyes and his right leg destroyed. You can read the details in my links.
Somehow he survived. But over the years, his traumatic brain injury (TBI) has morphed into schizophrenic-like thoughts and behavior. His power to reason vanished. His mother and his twin sisters Linda Privatte and Catherine J. Rippee-Hanson tended him in the family household for eighteen years, until his deformed brain turned him into a raging menace. He left the household and has made his way on the streets, where his sisters—both of whom have developed serious illnesses of their own—bring him food, clothing, canes. Vandals keep stealing all of it, and often also the money given him for food and other needs.
Why doesn’t somebody rescue Mark Rippee? Why doesn’t some agency . . . why doesn’t . . .
Those are very good questions, and I’m glad you asked them. But the answers are buried within the folds of incoherence that comprise so much of the American mental healthcare system. Or systems. Or “systems.”
Mark Rippee is a victim of a perfect storm of gothic bureaucracy. The pertinent bureaucrats at Solano County and California state levels have exhibited no discernible interest in finding any way to counter the bureaucratic snafus with a humane solution that would get this man into supervised care and treatment.
One might even say that they are hiding behind a “humane solution” that actually exists. This solution would begin with a declaration from a psychiatrist that Mark Rippee’s accident left his brain with “diminished capacity.” This ruling would permit Mark’s family to place him in an appropriate facility and/or to establish a conservatorship that would give them discretion over his affairs, including psychiatric care.
No dice: hospital psychiatrists have consistently, and weirdly, denied that Mark Rippee has “diminished capacity.”
And the reasoning behind this confounding denial? Well, it’s none of your business what the reasoning is. The hospital is protecting Mark Rippee’s rights, you see. Protecting them by way of the cartoonish Health Insurance Portability and Accountability Act. HIPAA was designed to ensure a patient’s “privacy.” “Privacy” that prohibits even family members from learning the medical procedures and condition of a patient. There’s an irony there, in case you missed it.
Catherine and Linda have fought tooth and claw, over parts of three decades, to tear through the self-serving laws and policies that keep Mark in a near-feral state. Two years ago, Catherine plunged into work on a petition in support of a California bill known as AB 1971. AB 1971 would have expanded the existing definition of “gravely disabled” to include medical treatment for a patient if the lack of treatment “may result in substantial physical harm or death.” It would have secured treatment for Mark Rippee. Catherine collected 82,000 signatures in favor of the petition.
In April 2018, the Disability Rights Education and Defense Fund, one of several lobbies that oppose conservatorship and deny other needs of the mentally ill, signaled that it disapproved of AB 1971. The California Hospital Association also weighed in on the negative side.
AB 1971’s sponsors pulled the bill.
The sisters’ determination would be the stuff of heroic legend, if we lived in a country that valued heroic legend. In the wake of Mark Rippee’s second brush with death by an oncoming car he couldn’t see, Catherine has released a new petition. It demands intervention from California Governor Gavin Newsom to rectify this travesty of public policy. It reads in part: “While we hold the County of Solano and many officials, departments and agencies responsible for not preventing this second tragedy that we told them would happen – We also demand that the State of California and in particular – Governor Gavin Newsom – whom we have previously attempted to contact – PAY ATTENTION TO THIS SITUATION and ACT accordingly!”
Moreover, thanks to the sisters and the Internet, word of Mark’s ordeal is spreading at the grass-roots level. Activists around the country, alerted to the nightmare, have begun writing letters demanding justice for Mark.
Here are two. Their tone of indignation and urgency is echoed by many more.
From Donna Erickson of Massachusetts:
“Hello, I’m writing to voice my concern, in regard to a homeless individual named James Mark Rippee. As you probably know, he is severely disabled both mentally and physically. Being blind only further complicates his poor condition. The real tragedy here is that none of this is his fault. Severe mental illness is a disease nobody chooses. Many who are afflicted are unaware of how sick they are, because of anosognosia, which is lack of insight, a condition that is a manifestation of the illness itself. It is not his fault that he repeatedly walks into traffic.
“His brain is broken, and he cannot see. Someone in this condition should never have been put on the street. So now he is hospitalized for another accident, resulting in critical injuries, including a skull fracture, brain bleed, and broken bones. He will need many surgeries.
“His family is devastated, because they tried so hard to get him off the streets. But the laws get in the way. This poor man requires a hospital, rehab, and eventually a long-term residential facility. If he is an elopement risk, then there are locked facilities. Mark’s value as a person is no less than any of us on Earth. He has fallen through the cracks of a very broken system.
“How would you feel if this was your family member? Mental illness can strike anyone. He is not a nobody. He is a family member of caring individuals who have tried everything in their power to help. The tragic part is that this all could have been avoided, if only someone had truly cared and listened. Keeping someone on the streets in his condition is disgraceful. And it shouldn’t matter what he says. He is unable to make a rational decision, which is in his best interest, due to his illness.
“The system has failed him, because no one intervened, even though the family had begged and pleaded. I had to voice my concern, because this could have been my son. This could have been anyone’s son, and we need to start taking care of our most vulnerable citizens!”
And from the Maryland advocate Laura Pogliano:
“My friend [Catherine] Hanson and her sister Linda Rippee have been trying to help their brother Mark for 13 years; a motorcycle crash left him with no eyes, a severe brain injury, broken bones all over his body, a metal rod in his leg, and as a result of TBI, schizophrenia. He’s been on the streets for years, being victimized, robbed, beaten and neglected. They’ve been denied help for him over and over by the county they’re in, by hospitals.
“He’s been admitted to, by group homes, by every support service you can think of. He was hit by a car a few months ago and while inpatient, one sister’s medical power of attorney was revoked, and the psychiatrist sided with his delusional raging patient, that he was capable of making his own medical choices and caring for himself (blind and floridly psychotic). He was discharged to a group home and lasted about a week.
“Now, living on the streets, Mark’s been hit by a car again! Only this time, he was thrown into the air and smashed his face against the driver’s windshield. He’s in bad shape, has another brain injury, the leg with the metal rods is shattered, his shoulder is dislocated and he might lose what’s left of his teeth.
“He’s going to need months of hospitals, multiple surgeries, and extended care. And guess what? He’s in the same damned hospital that battled back against his family and discharged him to the streets.
“Mental health care in America. You stand a slight, very slight chance of making it, if you’re healthy enough to ask for help and participate in it. If you’re really, really sick, you’re screwed.”
In a city in America, here in the Twenty-first century, a man has been left to die. But in America, the voices of reclamation are arising to insist on his right to live.
Bernie, you represent me in Congress. I am a constituent of yours who has voted for you regularly. We know one another a little. (In Vermont, everybody knows one another a little.) I have followed your political career with admiration. I have defended you against my Democrat and progressive friends who insist that you are prohibitively doctrinaire, headstrong, and abrasive/dismissive in conversation. (Who, knowing you, could possibly believe these things?!)
I applaud your decades of consistency in holding large corporations to account for their greed, deceptions, and perversions of economic and social justice. I feel inspired by your support of the American worker even as many American workers, including many in your home state, are blinded to your support by your self-identification as a “socialist.”
And so, when I make the urgent request that I am about to make, I hope you will not reject it out of hand as the trolling of a political opponent. I’m asking you to reconsider your stands on three critical elements of U.S. mental health-care policy. Singly and as a group, these elements in their present form contribute to the ongoing national crisis in the care of our most helpless citizens.
The three involve the so-called IMD exclusion, the HIPAA rules, and controversial laws surrounding the civil commitment of people in psychotic states.
Your problematic proposals are as follows: to defend the oppressive “IMD exclusion” that disallows Medicaid funding for those hospitalized with mental illness; to maintain the so-called HIPAA rule; and to keep in place the highly problematic civil commitment laws (laws that bar hospitalization of a person in a psychotic episode, unless it’s demonstrated that person is a danger to self or others).
Senator, each of these policies has caused untold and needless frustration, and often financial loss, to sufferers and their families. Each of the reform proposals you oppose amounts to a common-sense solution. Yet each, and all, of these laws are defended by lobbying groups within the anti-psychiatry community and by mental-illness deniers, despite breakthroughs in neuroscience and brain-scan technology dating to the 1980s.
To examine each of them:
The IMD (Institutions for Mental Diseases) exclusion bars federal Medicaid financing for patients in psychiatric facilities with more than sixteen beds. It was enacted in 1965, the new Bronze Age of mental-health care, when large, decrepit, and often brutally run asylums brooded over the landscape. In 2020, IMD is a destructive artifact that stands athwart the enlightened trend toward smaller, efficient community-based care centers with professionalized staffs.
Case in point: The venerable Brattleboro Retreat—Vermont’s largest psychiatric hospital—emblemizes the creaking policy’s noxious legacy: in January, the private nonprofit Retreat warned that a funding crisis might lead to its shutting down. Not until crisis negotiations a few weeks later between the governor and Vermont’s Agency of Human Services did the state grudgingly consent to cough up $2 million in emergency funds to keep the Retreat going. Its future remains precarious.
Meanwhile, Vermont’s shortage of acute care beds for the mentally ill has grown even more dire. In the words of the reform advocate DJ Jaffe, “It is hard for Senator Sanders to argue in favor of ‘healthcare for all’ while embracing the federally sanctioned discrimination embedded in Medicaid that is causing hospital beds for the seriously mentally ill to close.”
The cumbersome HIPAA is similarly a counter-productive policy that calls for scrapping, not defending. The Health Insurance Portability and AccountabilityAct was signed in 1996 to accomplish many things, most notably, to restrict the personal and medical data of hospital patients from scrutiny by insurance companies, employers, other care providers—and also from the patients’ family members.
The unintended consequences of HIPAA thrust mental patients’ families, into an abyss of anxiety and frustration. Denied any scrap of information—Is our child resting? Screaming? Lashing out at doctors? Improperly medicated? How can we help him/her?—parents can only rage against the curse-upon-curse that HIPAA imposes. My wife and I experienced this torture when our son Kevin was hospitalized with schizophrenia. We wanted desperately to know what medications he was being given. We had seen the horrifying effects on him from meds that did not suit his biological system and wanted to share what we knew.
Kevin was eventually released from the hospital. He took his life during an episode of psychosis a week before his twenty-first birthday in 2005.
Surely the HIPAA laws can at least be modified to include a sufferer’s loved ones in the information loop without releasing sensitive data to all and sundry. Yet, Senator Sanders, you have stated your opposition to any amendments whatsoever. Please—and I ask on behalf of desperate parents everywhere—please reconsider.
As for your intention to stand by the existing civil commitment laws: These laws changed the history of confronting psychotic behavior by raising, for the first time, legal obstacles to what had been intended as purely medical decisions. Most of these civil commitment laws were enacted by states in the 1970s, a period of passionate civil-rights activism and also fervent skepticism about the very existence of mental illness. The laws have bedeviled advocates and judges ever since. They address questions that have no clear answers, yet can determine the life or death of a person in a state of crisis, and of anyone nearby. Is this agitated person capable of self-harm or harm to others? Should such people be treated against their will, or should their civil liberties be prioritized above the risk of mayhem? And most critically, how is risk, or lack of it, ascertained in the emotionally charged moments of crisis? How is psychosis determined?
The commitment laws essentially allow the person in crisis to give the answers—a genuflection to the principle of civil liberties. These privilege the law above psychiatric/medical judgment. Given that civil liberties are among America’s most cherished ideals, this direction makes sense. Or it would make sense, if the person in psychosis is capable of reasoned thought.
Psychosis by definition is a break with reality, an inability to think in a rational way. In a large number of cases—up to 50%, according to most estimates—the affliction is accompanied by a condition called anosognosia, the inability to comprehend that one has a psychotic illness.
Given such overpowering impediments to clear thought, how can a sufferer possibly be expected to rule on his or her own need for psychiatric intervention?
DJ Jaffee, executive director of Mental Illness Policy Organization, offers one trending alternative: the use of assisted outpatient treatment (AOT). Jaffee writes, “AOT is a procedure that allows judges— after full due process— to commit the few seriously mentally ill who are historically and potentially dangerous to stay up to one year in outpatient treatment, often including medications, while they continue to live uninstitutionalized in the community. Outpatient commitment is less expensive and less restrictive than inpatient commitment.”
Dj Jaffe
I’m not suggesting that any of these remedies is simple. Nothing about mental illness is simple. It remains a unique curse, defying cure, reclamation, policies without pitfalls. All who attempt to seriously tackle these challenges must brace for unintended consequences. Yet these hurdles are no excuse for allowing patently bad policies to continue unopposed.
We in the advocacy movement are grateful for your political leadership in the struggle for justice and thoughtful reform in our broken mental healthcare system, Senator Sanders. Please consider these suggestions for critical refining of your policies in your campaign.
“There is a crime here that goes beyond denunciation. There is a sorrow here that weeping cannot symbolize. There is a failure here that topples all our success.”
John Steinbeck
Vacaville, California, has a history of popular uprisings to confront the powerful as they violate the humanity of the dispossessed.
In 1932, organizers came to Vacaville to organize the Cannery and Agricultural Workers’ Industrial Union, which fought the starvation-wage exploitation of farm and orchard laborers by the state’s powerful growers. The CAWIU went on strike that December–one of 140 strikes, some of them violent, that occurred between 1930 and 1939. These actions caught the attention of John Steinbeck, and triggered his impulse to write The Grapes of Wrath, which won the Pulitzer Prize in 1940 and contributed to his Nobel Prize for Literature in 1962.
Now Vacaville finds itself at the tipping-point of another defining moral struggle pitting society’s outcasts against entrenched power. The outcasts in the current showdown, the homeless mentally ill, are represented by James Mark Rippee, the blind, gravely brain-damaged street dweller of whom I’ve written extensively on this blog. The power centers that control his fate are the extravagantly named Kaiser Permanente Vacaville Medical Center, and the Solano County Board of Supervisors.
James Mark Rippee – Photo Courtesy Linda Privette
On Tuesday, October 8 (tomorrow, as I write this) one or both these institutions will render decisions that will either end Mark’s twelve years of unimaginable suffering on the small city’s streets, or cast him back into the chaos and brutality of those streets as if he were a leper from the slums of New Dehli.
Mark Rippee. Photo Courtesy CJ Hanson.
Mark Rippee is 56 now; emaciated, sickly, and delusional, as he has been since the motorcycle accident in 1987 that cost him his vision, crippled him, and left bits of his brain scattered in an alfalfa field.
Winter is coming on. Mark has routinely been beaten and robbed over the years by random thugs who have taken a succession of walking sticks his sisters have provided him, as well as blankets that have been his only insulation against the cold.
Mark Rippee
His age and failing health augur against his surviving the cold months out-of-doors one more time. The ongoing, unfathomable indifference of the County board to his physical exposure, and the equally bewildering failure of Kaiser Permanente’s psychiatrists to find anything wrong with his psyche, augur against his rescue by those whose charge is the public health and safety.
The “policy” decisions on October 8 at the Kaiser Permanente Vacaville Medical Center and the Solano County Board of Supervisors, then, probably amount to a life-or-death sentence for James Mark Rippee. “Policy” explains why Mark Rippee remains homeless. The pertinent “policies” ensnarled in the maimed reasoning of brain-damage victims and in the equally maimed consciences of bureaucrats. “Policies” have constricted his sisters, Linda Privatte and C.J. Hanson, as they have struggled to gain simple shelter and medical care for their brother, whose fog of reasoning blocks him from giving necessary consent.
Mark is in the hospital because on September 14 he stumbled into traffic and was hit by a car as he wandered blindly along Monte Vista Avenue in Vacaville. The impact knocked his head against the concrete and re-opened an abcess. The pain overcame his delusional resistance to being hospitalized or treated (a common resistance, known as “anosognosia,” or lack of insight, in schizophrenia victims).
Mark Rippee’s hospital stay seems likely to end on October 8, when the Kaiser Permanente Vacaville Medical Center will release him to–well, it will release him. It is not the “policy” of the Kaiser Permanente Vacaville Medical Center to give much of a rap where patients such as Mark Rippee end up. “Policy,” you see, allows no moral dimension. It normally is accompanied, however, by a burning desire not to spend money.
And on this same day the bureaucracy known as the Solano County board of supervisors will hold yet another hearing to hear opinion on whether Mark Rippee’s sisters should, at last, be granted a conservatorship that would allow them to make decisions on his behalf. Conservancy, like hospital and psychiatric care, requires the expenditure of money. Such money is sometimes available through state and federal government. But then there is that annoying matter of consent by the patient.
One thing will be different, in Mark Rippee’s favor, on this Tuesday. Public opinion is at last beginning to coalesce in his favor. The sisters’ exhaustive efforts at rallying community support have started to pay off, in the form of rallies and an expected turnout at the supervisors’ hearing. Advocates around the country are on standby, alerted by Facebook postings. A T-shirt is available for purchase online. It bears Mark’s ravaged likeness and the declaration that he blurted out, surprising everyone, during his recuperation. It should serve as a manifesto for all his brothers and sisters on this country’s streets:
“I am NOT homeless! I have a home! My home is the United States of America!”
Mark James Rippee
On Tuesday, October 8, we will see whether the United States of America fulfills Mark Rippee’s cry of trust.
The good news is that President Trump wants to do something about homeless Americans on the streets.
The bad news is that President Trump wants to do something about homeless Americans on the streets.
On Monday, newspapers and television networks broke the news that the President of the United States, whose name is Donald Trump, had at last swiveled the full attention of his very, very large brain to one of the most appalling crises confronting American cities: the crisis of homeless people on the streets.
Social scientists and others of sadly lesser intellect have noticed the crisis as well, of course, and analyzed it to the best of their limited ability: as a vast ongoing human calamity with dire implications for public health (the containment of hepatitis and opioid epidemics, for example); community and family stability, criminal justice and law enforcement, the control of dangerous drugs, productivity and the employment base.
These are vitally important but largely utilitarian considerations. They do not contemplate the profound moral/religious dimension of this malady: the obligation to reclaim disintegrating human lives.
Few agents of disintegration are more darkly effective than mental illness–serious mental illness (incurable brain diseases such as schizophrenia) in particular. A 2015 survey by the The U.S. Department of Housing and Urban Development, the latest available, reported that of the nearly 565,000 people who were homeless on a given night, fully one-quarter, or 140,000, suffered from a S.M.I. (Serious Mental Illness). Nearly half, or 250,000, were in the grip of some sort of mental disorder.
S.M.I. victims, their reasoning powers diminished or gone, are essentially helpless on the streets. Cut off from providers of stabilizing medication, they are prey to robbers, thugs, thieves, and sometimes rogue police officers. On rare occasions, they become predators as well: upon others, and upon themselves, via suicide.
That is the context of the societal predicament which, nearly three-fourths of the way through his term of office, has activated the engines of President Donald Trump’s very large intellect.
It is clear from this interview that Donald Trump does not see homelessness as a social-justice problem or a humanitarian problem. He sees it as a cosmetic problem. One that “started two years ago [sic]”
It is further clear that the homeless are inconveniences. Disgraceful pests who make beat-walking police officers sick. “I mean actually they’re getting very sick.” They are affronts to civic pride: human (or semi-human) obstacles to decent upstanding work-loving citizens. The homeless make it very difficult for office-workers to get to work, you see, and thus are ruining our cities. “You have people that work in those cities,” Donald Trump revealed to his pal Tucker Carlson not long ago. “They work in office buildings. And to get into the building, they have to walk through a scene that nobody would have believed possible three [sic] years ago.”
–And let Donald Trump tell you something: the threats posed by the homeless reach far beyond those that menace nauseated beat-cops and nimble-toed office workers. The homeless strike at the very foundations of America’s might. Take Washington, D.C. (before Donald Trump got in): “When we have leaders of the world coming in to see the President of the United States and they’re riding down the highway . . . they can’t be looking at that [sic]. I really believe that it hurts our country.”
–Don’t get Donald Trump wrong. Nobody is more ruefully forgiving of the barbaric horde than Donald Trump. “San Francisco–I own property in San Francisco; I don’t care, except it was so beautiful.”
–Because, you see, Donald Trump is very, very educated about mental illness: In fact nobody knows more about mental illness than Donald Trump: ” . . . the people living [on the streets] are living in hell, too . . . although some of them have mental problems where they don’t even know they’re living that way; but perhaps they like living that way.” (Emphasis added)
No doubt! Just like those African slaves in the antebellum South were “happy with their situation,” as my innocently bigoted mother used to assure me.
–But not to worry. Donald Trump’s very large, very beautiful mind has not only identified the issue at the heart, as it were, of the homeless problem: bad cosmetics. He has fingered, as it were, the Masters of Evil responsible for the atrocity. “And this is the liberal establishment . . . When you look at some of these, they’re usually sanctuary cities, they’re run by very liberal people, and the states are run by very liberal people.”
–Donald Trump has clashed with these evil forces before–and sent them packing with a strategy that was stellar in its simplicity. “When I first became president, we had certain areas of Washington, D.C., where that was starting to happen. And I ended it very quickly; I said, ‘You can’t do that.'”
–And now Donald Trump is poised to expand that breathtaking solution into a national plan of action. As he told Tucker in the July 1 Fox News interview I have been drawing on here: “So, we’re looking at it very seriously. We may intercede. We may do something to get that whole thing cleaned up. It’s inappropriate [!]. Now, we have to take the people, and do something. We have to do something.”
Take what people where? And do what? one wonders with a shudder. The loyal Tucker Carlson didn’t ask, and Donald Trump didn’t say. But the national press, those damned “enemies of the people,” did not wait for the president’s second-favorite cliche, “You’ll see.” They checked some sources. Here are some of the headlines that resulted on Monday:
Trump pushing for major crackdown on homeless camps in California, with aides discussing moving residents to government-backed facilities (The Washington Post)
Trump Reportedly Wants to Destroy Homeless Camps in California. Officials Say He Doesn’t Have a Clue.(Vice)
Trump officials look to fix California homeless problem, state officials say back off (USA TODAY)
“My first reaction is that it felt like internment camps for people experiencing homelessness. The president doesn’t seem to have any grasp of the homeless crisis not only in California but around the country.”
It doesn’t take a very, very big brain to suss out Donald Trump’s entire, unabridged spectrum of thought about mental illness. (1) He does not know diddly-squat about the disease. (2) He doesn’t care diddly-squat about its victims. And (3) coming as they do from the lips of a self-styled “man of the people,” Donald Trump’s remarks are about as consummately elitist and plutocratic as you are ever likely to hear outside the Clarence Day Room of the Yale Club.
If you are homeless and mentally ill–hell, if you are homeless, period–you are to Donald Trump as a speck of acne on the Ivanka-like face of America.
You are an impediment; an inconvenience; an ugly flaw to be hidden under a cosmetic treatment. (The “cosmetic treatment” in this case seems to require “facilities.” Camps. And this much is true: Donald Trump does know a little about camps.)
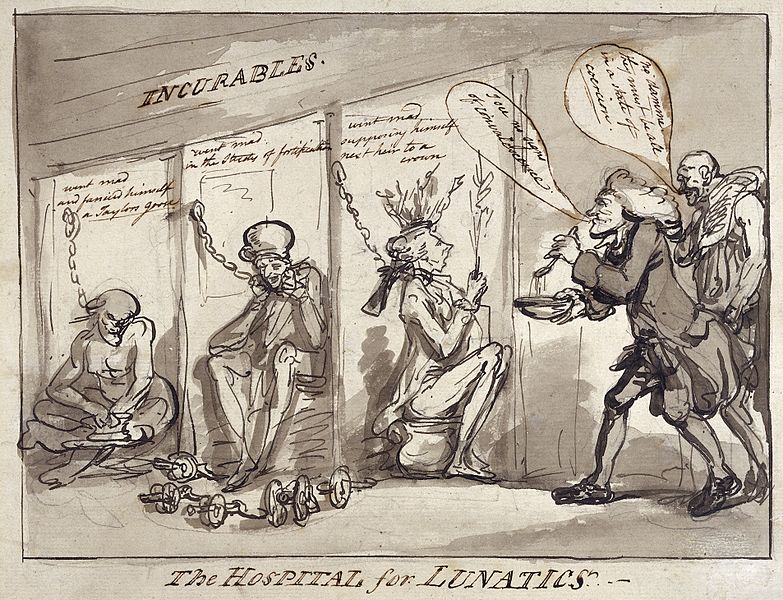
But in a darkly intuitive way, Donald Trump may know what he is doing. Rounding up homeless m.i. victims and sweeping them away out of sight behind walls and locked doors would place his aims squarely on a plane with history’s first institution designed to, let us say, cosmeticize urban streets of “lunaticks,” “morons,” and “idiots”: the notorious Bedlam Asylum in London, which opened for business in the 13th century and brutalized generations of “patients” until it was closed in 1815.
Of course, that sort of barbarism is unthinkable in enlightened, humane, modern-day America. As unthinkable as separating small refugee children from their parents at our southern border and placing them in cages.
In case you thought I was making up or paraphrasing the Donald Trump quotes above, please carefully review the clip I posted above, from his July 1 interview with Tucker Carlson.
My next blog will focus on the impending public-policy threats–and promises–vis-a-vis the homeless population.
The leading Democratic candidates for president in 2020 have at long last agreed that abolishing this atrocity is an essential part of criminal-justice reform. It is up to us to hold them to their words.
When you hear or read the words “solitary confinement,” what images form in your mind?
A naughty inmate spending some time in a kind of “time out” space wearing a hang-dog expression?
A lonely prisoner in a tiny dark cell gazing at light from the slit of a window, with maybe half a bowl of dirty drinking water at his feet?
A mentally ill man who, after 112 consecutive days of solitary, has just severed his penis with a razor and flushed it down his cell’s toilet?
One of these things is not like the others.
All three images are rooted in the dark dominion of solitary confinement. Only one of them burns through the fog of euphemism and forces a reckoning with a terrible truth—in this case, one of the most perverse, destructive, and unnecessary varieties of soul-murder yet devised by man.
The topic “solitary confinement” has been raised lately (and gingerly, and fleetingly) by several candidates for the 2020 Democratic presidential nomination: raised as an agenda item in their calls for repairing the fissures in America’s criminal-justice system. (Criminal-justice reform is tightly intertwined with reform of our negligent systems of mental healthcare in America.)
Dorothea Dix
The candidates have in turn been influenced—inspired—by the efforts of a bright new coalition of mental-health reform advocates: parents, mostly, spurred to action by the death or deep psychosis of a beloved child. Polite yet unyielding, ferociously informed, they amount to a neo-Dorothea Dix approach to getting justice for the dispossessed.
Iowa is their perfectly chosen beachhead. Not only does the state offer an early concentration of corndog-chewing candidates for them to buttonhole. Iowa City is the home of the turbo-charged advocacy team of Scott and Leslie Carpenter. Armed with an exhaustive five-point bill of particulars for mental healthcare reform compiled by the California advocate DeDe Moon Ranahan, the Carpenters essentially have brought the grass roots onto equal footing with the political elite—on this issue, at least.
But why shine the spotlight on solitary confinement when the justice reform agendas are crowded with so many other “big-ticket” demands? Cutting the U.S. prison population in half comes to mind, as do ending the notorious “cash bail” system that keeps poor young inmates locked up only because they can’t afford otherwise; or tightening up on police oversight; or legalizing marijuana; or abolishing private prisons.
Here is the reason: I sense that of all these important, difficult-to-achieve goals, the abolishing of solitary is among the easiest to bring up and then dismiss: the one most vulnerable to lip service.
Thomas Edward Silverstein
And that would be a colossal shame. Stuffing sentient human beings into small, dark, fetid enclosures and leaving them there is about the worst thing it is possible to do to one’s fellow man. The American record for duration in solitary was held by a triple murderer named Thomas Silverstein, who died just last May at age 67. He’d spent more than half his life in isolation.
It borders on the impossible to find shared humanity with a monster like Silverstein. Yet traces of his humanity struggle to declare themselves like green shoots through cracked pavement. “It’s almost more humane to kill someone immediately than it is to intentionally bury a man alive,” he wrote. For one superb writer’s searching attempt, read Pete Earley’s masterful 1992 book, The Hot House: Life Inside Leavenworth Prison.
Or return for a moment to the lost soul who severed his penis with a razor. That would be the mentally ill inmate identified by his initials, J.I., a solitary inmate at Broward County Jail in Fort Lauderdale, Florida. On the night of September 2018, jail guards, alerted by prisoners’ shouting in a lockdown unit, rushed to the scene, where they beheld J.I., his hands and forearms bloody, who told them: “I have a real medical emergency. I just cut my penis off and flushed it down the toilet. I have no need for it anymore.”
Solitary is patently barbaric; bereft of any use (other than convenience and a lust for inflicting psychic pain). It is a legalized yet likely unconstitutional torture which, I have come to believe, is slightly more heinous even than the death penalty: its victims, while not dead, experience death as their own observers, existing in claustrophobic isolation and silence and darkness and decay, with no definable release awaiting them.
And so in order to tolerate it as public policy or even as a thought, some self-anesthetizing helps. (Those charged with actually imposing it on human beings presumably develop tougher psychic scar tissue.) “Solitary confinement” is a term useful for the necessary numbing: an abstraction, one of those “Orwellian” constructions that serve more to camouflage than to evoke their full, and usually terrifying implications.
That very abstraction is dangerous. It can too easily lead to evaporation.
This blog, then, is a plea to those presidential candidates who have made the abolition of solitary confinement a part of their criminal-justice reform demands: Do not let this happen. Honor the constituency that has materialized in Iowa and exists throughout the nation. Keep this issue alive.
In subsequent blogs I will trace the peculiar origins of solitary confinement in America, and will look into some of the lesser-known forms of its use—for example, as an instrument of control for juvenile inmates and even schoolchildren.
I will close this blog with a soaring testimony of hope, resilience, faith, and self-reclamation written by a former criminal and solitary inmate named Thomas Tarrants, and published in the August 19 edition of Christianity Today. [efn_note] I Was a Violent Klansman Who Deserved to Die [/efn_note] It was sent to me by my friend, the literary scholar Harold K. Bush of St. Louis University. Thank you, amigo.
Two mobilizations of historic enlightened reform are abruptly converging in American politics and policy. Their aims are intertwined: to bulldoze and rebuild our blighted structures of criminal justice, and to reclaim our dispossessed mentally ill brothers and sisters from the hellscape of danger, pain, and early death that the blight of justice confers on them. And the economic drain that it exacts from all of us.
The symbiotic forces are (1) the elite tier of progressive candidates for the 2020 presidential election, and (2) the sleeves-up cadre of activists working at Ground Zero who toil because they daily confront serious mental illness up close, and witness its effects for what they are: cancers upon our societal health and sense of decency.
(The first of two parts)
At first glance, justice and mental-healthcare reform may seem but a marginal sliver of all the issues pressing in on America in the 2020 elections. (The physical salvation of the planet comes to mind, and abolishing the immigrant gulags at our southern border.)
This is a distorted, damaging perception, made more dangerous because the crisis is so easily concealed. It can sometimes seem as though insanity and incarceration are like two undersea predators, their tentacles wrapped around each other in a death-struggle of futility. The quality of courts, jails, and prisons has been weakened by years of tending people who should be under psychiatric care. The essentially helpless 11.2 million seriously mentally ill population in turn is vulnerable to suffocation in the folds of feckless court rulings and inhumane treatment behind bars, including deprivation of essential meds and the beckoning maw of solitary confinement (about which more—much more—later.) The one in five adults with less chronic afflictions—nearly 47 million—are within range of the tentacles as well.
Yet that perception, or lack of perception, prevails. It prevails because to open our eyes to the full truth of these abominations is to risk scorching the soul. “I’ll do what little I can in writing,” lamented the great James Agee in another, and again oddly similar context some 75 years ago. “Only it will be very little. I’m not capable of it; and if I were, you would not go near it at all. For if you did, you would hardly bear to live.”
Thus we banish the ghastly effects from our attention as “normal” Americans, until it is too late. The entwined crises strike quickly, and from nowhere, and spread ruin: in households and communities (black and poor ones especially), in the workplace, in public places, in our economic state, and in the less tangible spheres of our collective optimism, hope, and peace of mind.
America has needed an “intervention” for more than two centuries. Intervention seems, at last, to be on its way.
To review the Democrats’ reform plans:[efn_note] I have drawn on several sources, including the candidates’ websites and the excellent summarizing of Vox’sGerman Lopez, in this essay.[/efn_note]
Pete Buttigieg photo credit: Gage Skidmore
The most ambitious manifestos, in my unscientific reckoning, were issued within the last ten days by Senators Bernie Sanders and Elizabeth Warren and South Bend, Indiana Mayor Peter Buttigieg. Nearly as powerful were the earlier justice reform announcements of Cory Booker, Amy Klobuchar, and Julian Castro. Joe Biden and Kamala Harris submitted strong, if not notably comprehensive, reform ideas.
This ranking hierarchy is not as fixed as the tiers might imply. The eight plans are far more significant for their overlapping reform goals they stress than for their differences.
Elizabeth Warren
Slashing into federal prison glut is high on most lists. Sanders, Warren and Buttigieg unveiled proposals that would cut into mass-incarceration, each by roughly 50 percent: by reducing long sentences, ending the “cash bail” system that pauperizes poor families of those arrested, tightening up on police oversight, legalizing marijuana, and abolishing private prisons. Sanders’s document, at 6000 words, is by far the most minutely detailed. Warren would go after policies that “criminalize” homelessness, poverty, and mental health problems (critically, she has not elaborated on this last). Booker would scale back inmate numbers via a clemency program that would free many elderly inmates under the theory that criminals “age out” of their impulses to commit violent crimes. Klobuchar also embraces clemency via a restructured reform plan and would modify the “tough-on-crime” stances she held as a prosecutor in Minnesota.
Julián Castro
Castro’s vision is likewise far-ranging, but he places special emphasis upon overhauling violent and clueless behavior of policemen. He wants to curb the use of force, end stop-and-frisk, holding police more accountable for misconduct, and restoring trust among police and the communities they are sworn to protect.
As for Biden and Harris, their reform plans are similarly comprehensive and replicate the bold ideas of their rivals as listed above. Both candidates—and to some extent Klobuchar as well—are preoccupied with freeing themselves from the taint of the “tough-on-crime” stances that they adopted in the mid-1990s.
That is my personal survey, unfairly truncated perhaps, of the generally ground-breaking flurry of criminal-justice reform ideas released by eight of the leading progressive presidential candidates.
An obvious but important caveat: none of these audacious ideas will tap-dance its way into law or policy should its sponsor get elected. (The proto-autocrat decrees of our current incumbent might lull some into that assumption.) A new chief executive will need to inspire the House and Senate to a pitch of pro-active fervor not seen since the First Hundred Days of Franklin D. Roosevelt’s presidency when the New Deal took form in a blizzard of “relief, recovery, and reform.” For our present stumbling and divided Congress to suddenly sprout capes, masks, and flippers and get busy cleaning out the present rot may seem a stretch. Yet things can happen quickly, as the last midterms showed, and a whiff of activism does linger in the air.
With all this in mind, let us turn to the symbiotic manifesto that has arisen from those ordinary heroes at Ground Zero: “Grassroots 2020: A 5-Part Plan for Mental Illness SMI.”
Grassroots: 2020 has been personally distributed to visiting Democratic candidates or mailed to their offices by Leslie and Scott Carpenter of Council Bluffs, Iowa. The Carpenters’ tireless work has helped join the reformist trajectories of these politicians and the people.
I lay it out below with minimal editing, in summary form. You will note that each part of the plan delineates action that a president can undertake, sometimes independently of Congress. And unlike the candidates’ ideas above, Grassroots: 2020 addresses justice-reform issues (incarceration-trimming, for example) only incidentally. It focuses on existing rules, many of them arcane to the non-specialist, that nonetheless have caused decades of frustration and despair for those struggling to reclaim their afflicted loved ones from a decayed system:
A FIVE-PART PLAN TO ADDRESS SERIOUS MENTAL ILLNESS (SMI) 2020 PRESIDENTIAL CANDIDATES. PLEASE ADDRESS THESE TOPICS IN YOUR CAMPAIGN APPEARANCES AND DEBATES:
1. RECLASSIFY SERIOUS MENTAL ILLNESS (SMI) FROM A BEHAVIORAL CONDITION TO WHAT IT IS – A NEUROLOGICAL MEDICAL CONDITION
WHY RECLASSIFICATION IS IMPORTANT:
Re-classification will unlock more research funding and help eliminate discrimination in treatment, insurance reimbursement, and the perception of SMI as a “behavioral” condition. SMI is a human rights issue. The National Institutes of Mental Health ranks SMI among the top 15 causes of disability worldwide with an average lifespan reduction of 28 years.
PRESIDENTIAL ACTION:
• Create a cabinet position exclusively focused on SMI. • Push for Congressional appropriations to include schizophrenia in a CDC[efn_note]The federal Centers for Disease Control Institute[/efn_note] program that collects data on the prevalence and risk factors of neurological conditions in the U.S. population.
Overly strict HIPAA laws make it extremely difficult for families and caregivers to partner in the treatment of their loved ones, resulting in important life-saving medical information gaps. By eliminating this barrier, family support will be strengthened, reducing the chance of relapse, homelessness, imprisonment, and death.
PRESIDENTIAL ACTION:
Work with legislators to change HIPAA law to ensure mental health professionals are legally permitted to share and receive critical diagnostic criteria and treatment information with/from parents or caregivers of SMI.
3. REPEAL MEDICAID’S INSTITUTES FOR MENTAL DISEASE EXCLUSION (IMD).
WHY IMD REPEAL IS IMPORTANT:
The Medicaid IMD Exclusion prohibits Medicaid payments to states for those receiving psychiatric care in facilities with more than 16 beds for those in the 21-65 age group. This demographic represents the majority of SMI cases. Repeal of the IMD Exclusion will increase the availability of acute care, inpatient psychiatric beds. The IMD exclusion not only discriminates against those suffering from neurological brain disorders, it’s a leading cause of our national psychiatric hospital bed shortage.
PRESIDENTIAL ACTION:
• Work with legislators to repeal the IMD exclusion.
4. PROVIDE A FULL CONTINUUM OF CARE FOR THOSE WITH SMI
WHY A FULL CONTINUUM OF CARE IS IMPORTANT:
A continuum of care insures that SMI patients receive early intervention at all stages of their illnesses, long-term care when needed, and follow-up treatment (medications and therapies) when they’re released. Providing a continuum of care reduces: incarcerations, emergency rooms visits, homelessness, and death. A continuum of care provides life-time management that permits a patient to move without penalty from one level of care to another as needed.
PRESIDENTIAL ACTION:
• Create federal incentives to states which are addressing a full array of inpatient, outpatient, and supportive housing care.
5. DECRIMINALIZE SERIOUS MENTAL ILLNESS (SMI)
WHY DECRIMINALIZATION OF SMI IS IMPORTANT:
People suffering with other neurological conditions like Alzheimer’s and dementia can get treatment promptly without being kicked out of their homes to wander the streets until they are arrested and put in jail or prison rather than a hospital. Serious mental illness is the only disease where the doors to treatment are shut unless a crime is committed. This is pure and simple discrimination with the disastrous results we see in our country today — homelessness, incarceration, the disintegration of families, and death.
PRESIDENTIAL ACTION:
• Work with legislators to change “must be a danger to self or others” criteria. • Work with legislators to change involuntary commitment criteria, alleviating the subjective nature of “gravely disabled” and redefining it in objective terms based on scientific medical need for treatment. Psychosis, like a stroke, is a traumatic brain injury and needs immediate treatment for the best outcome.
Bernie Sanders
Returning to the candidates’ manifestos, I have omitted two demands that show up in most of them, yet are given no more than lip-service by none except Bernie Sanders: abolishing capital punishment and solitary confinement. Both are urgent. Deciding which is the most urgent depends, I guess, upon the morbid calculation of whether continued existence in the “hole,” with its barbaric history of destroying human personality, is worth the torture. I have felt my way to an agonizing decision. In my next blog I will urge the candidates to meditate on solitary confinement for exactly what it is, and to treat it as primary target for abolishment.


























.jpg){kind=link}