The leading Democratic candidates for president in 2020 have at long last agreed that abolishing this atrocity is an essential part of criminal-justice reform. It is up to us to hold them to their words.
When you hear or read the words “solitary confinement,” what images form in your mind?
A naughty inmate spending some time in a kind of “time out” space wearing a hang-dog expression?
A lonely prisoner in a tiny dark cell gazing at light from the slit of a window, with maybe half a bowl of dirty drinking water at his feet?
A mentally ill man who, after 112 consecutive days of solitary, has just severed his penis with a razor and flushed it down his cell’s toilet?
One of these things is not like the others.
All three images are rooted in the dark dominion of solitary confinement. Only one of them burns through the fog of euphemism and forces a reckoning with a terrible truth—in this case, one of the most perverse, destructive, and unnecessary varieties of soul-murder yet devised by man.
The topic “solitary confinement” has been raised lately (and gingerly, and fleetingly) by several candidates for the 2020 Democratic presidential nomination: raised as an agenda item in their calls for repairing the fissures in America’s criminal-justice system. (Criminal-justice reform is tightly intertwined with reform of our negligent systems of mental healthcare in America.)
Dorothea Dix
The candidates have in turn been influenced—inspired—by the efforts of a bright new coalition of mental-health reform advocates: parents, mostly, spurred to action by the death or deep psychosis of a beloved child. Polite yet unyielding, ferociously informed, they amount to a neo-Dorothea Dix approach to getting justice for the dispossessed.
Iowa is their perfectly chosen beachhead. Not only does the state offer an early concentration of corndog-chewing candidates for them to buttonhole. Iowa City is the home of the turbo-charged advocacy team of Scott and Leslie Carpenter. Armed with an exhaustive five-point bill of particulars for mental healthcare reform compiled by the California advocate DeDe Moon Ranahan, the Carpenters essentially have brought the grass roots onto equal footing with the political elite—on this issue, at least.
But why shine the spotlight on solitary confinement when the justice reform agendas are crowded with so many other “big-ticket” demands? Cutting the U.S. prison population in half comes to mind, as do ending the notorious “cash bail” system that keeps poor young inmates locked up only because they can’t afford otherwise; or tightening up on police oversight; or legalizing marijuana; or abolishing private prisons.
Here is the reason: I sense that of all these important, difficult-to-achieve goals, the abolishing of solitary is among the easiest to bring up and then dismiss: the one most vulnerable to lip service.
Thomas Edward Silverstein
And that would be a colossal shame. Stuffing sentient human beings into small, dark, fetid enclosures and leaving them there is about the worst thing it is possible to do to one’s fellow man. The American record for duration in solitary was held by a triple murderer named Thomas Silverstein, who died just last May at age 67. He’d spent more than half his life in isolation.
It borders on the impossible to find shared humanity with a monster like Silverstein. Yet traces of his humanity struggle to declare themselves like green shoots through cracked pavement. “It’s almost more humane to kill someone immediately than it is to intentionally bury a man alive,” he wrote. For one superb writer’s searching attempt, read Pete Earley’s masterful 1992 book, The Hot House: Life Inside Leavenworth Prison.
Or return for a moment to the lost soul who severed his penis with a razor. That would be the mentally ill inmate identified by his initials, J.I., a solitary inmate at Broward County Jail in Fort Lauderdale, Florida. On the night of September 2018, jail guards, alerted by prisoners’ shouting in a lockdown unit, rushed to the scene, where they beheld J.I., his hands and forearms bloody, who told them: “I have a real medical emergency. I just cut my penis off and flushed it down the toilet. I have no need for it anymore.”
Solitary is patently barbaric; bereft of any use (other than convenience and a lust for inflicting psychic pain). It is a legalized yet likely unconstitutional torture which, I have come to believe, is slightly more heinous even than the death penalty: its victims, while not dead, experience death as their own observers, existing in claustrophobic isolation and silence and darkness and decay, with no definable release awaiting them.
And so in order to tolerate it as public policy or even as a thought, some self-anesthetizing helps. (Those charged with actually imposing it on human beings presumably develop tougher psychic scar tissue.) “Solitary confinement” is a term useful for the necessary numbing: an abstraction, one of those “Orwellian” constructions that serve more to camouflage than to evoke their full, and usually terrifying implications.
That very abstraction is dangerous. It can too easily lead to evaporation.
This blog, then, is a plea to those presidential candidates who have made the abolition of solitary confinement a part of their criminal-justice reform demands: Do not let this happen. Honor the constituency that has materialized in Iowa and exists throughout the nation. Keep this issue alive.
In subsequent blogs I will trace the peculiar origins of solitary confinement in America, and will look into some of the lesser-known forms of its use—for example, as an instrument of control for juvenile inmates and even schoolchildren.
I will close this blog with a soaring testimony of hope, resilience, faith, and self-reclamation written by a former criminal and solitary inmate named Thomas Tarrants, and published in the August 19 edition of Christianity Today. [efn_note] I Was a Violent Klansman Who Deserved to Die [/efn_note] It was sent to me by my friend, the literary scholar Harold K. Bush of St. Louis University. Thank you, amigo.
Two mobilizations of historic enlightened reform are abruptly converging in American politics and policy. Their aims are intertwined: to bulldoze and rebuild our blighted structures of criminal justice, and to reclaim our dispossessed mentally ill brothers and sisters from the hellscape of danger, pain, and early death that the blight of justice confers on them. And the economic drain that it exacts from all of us.
The symbiotic forces are (1) the elite tier of progressive candidates for the 2020 presidential election, and (2) the sleeves-up cadre of activists working at Ground Zero who toil because they daily confront serious mental illness up close, and witness its effects for what they are: cancers upon our societal health and sense of decency.
(The first of two parts)
At first glance, justice and mental-healthcare reform may seem but a marginal sliver of all the issues pressing in on America in the 2020 elections. (The physical salvation of the planet comes to mind, and abolishing the immigrant gulags at our southern border.)
This is a distorted, damaging perception, made more dangerous because the crisis is so easily concealed. It can sometimes seem as though insanity and incarceration are like two undersea predators, their tentacles wrapped around each other in a death-struggle of futility. The quality of courts, jails, and prisons has been weakened by years of tending people who should be under psychiatric care. The essentially helpless 11.2 million seriously mentally ill population in turn is vulnerable to suffocation in the folds of feckless court rulings and inhumane treatment behind bars, including deprivation of essential meds and the beckoning maw of solitary confinement (about which more—much more—later.) The one in five adults with less chronic afflictions—nearly 47 million—are within range of the tentacles as well.
Yet that perception, or lack of perception, prevails. It prevails because to open our eyes to the full truth of these abominations is to risk scorching the soul. “I’ll do what little I can in writing,” lamented the great James Agee in another, and again oddly similar context some 75 years ago. “Only it will be very little. I’m not capable of it; and if I were, you would not go near it at all. For if you did, you would hardly bear to live.”
Thus we banish the ghastly effects from our attention as “normal” Americans, until it is too late. The entwined crises strike quickly, and from nowhere, and spread ruin: in households and communities (black and poor ones especially), in the workplace, in public places, in our economic state, and in the less tangible spheres of our collective optimism, hope, and peace of mind.
America has needed an “intervention” for more than two centuries. Intervention seems, at last, to be on its way.
To review the Democrats’ reform plans:[efn_note] I have drawn on several sources, including the candidates’ websites and the excellent summarizing of Vox’sGerman Lopez, in this essay.[/efn_note]
Pete Buttigieg photo credit: Gage Skidmore
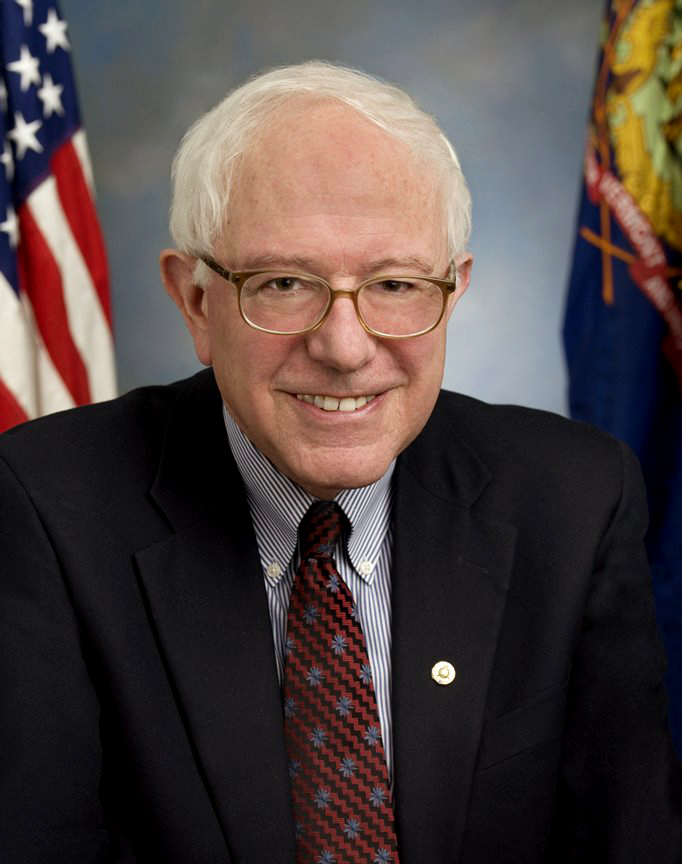
The most ambitious manifestos, in my unscientific reckoning, were issued within the last ten days by Senators Bernie Sanders and Elizabeth Warren and South Bend, Indiana Mayor Peter Buttigieg. Nearly as powerful were the earlier justice reform announcements of Cory Booker, Amy Klobuchar, and Julian Castro. Joe Biden and Kamala Harris submitted strong, if not notably comprehensive, reform ideas.
This ranking hierarchy is not as fixed as the tiers might imply. The eight plans are far more significant for their overlapping reform goals they stress than for their differences.
Elizabeth Warren
Slashing into federal prison glut is high on most lists. Sanders, Warren and Buttigieg unveiled proposals that would cut into mass-incarceration, each by roughly 50 percent: by reducing long sentences, ending the “cash bail” system that pauperizes poor families of those arrested, tightening up on police oversight, legalizing marijuana, and abolishing private prisons. Sanders’s document, at 6000 words, is by far the most minutely detailed. Warren would go after policies that “criminalize” homelessness, poverty, and mental health problems (critically, she has not elaborated on this last). Booker would scale back inmate numbers via a clemency program that would free many elderly inmates under the theory that criminals “age out” of their impulses to commit violent crimes. Klobuchar also embraces clemency via a restructured reform plan and would modify the “tough-on-crime” stances she held as a prosecutor in Minnesota.
Julián Castro
Castro’s vision is likewise far-ranging, but he places special emphasis upon overhauling violent and clueless behavior of policemen. He wants to curb the use of force, end stop-and-frisk, holding police more accountable for misconduct, and restoring trust among police and the communities they are sworn to protect.
As for Biden and Harris, their reform plans are similarly comprehensive and replicate the bold ideas of their rivals as listed above. Both candidates—and to some extent Klobuchar as well—are preoccupied with freeing themselves from the taint of the “tough-on-crime” stances that they adopted in the mid-1990s.
That is my personal survey, unfairly truncated perhaps, of the generally ground-breaking flurry of criminal-justice reform ideas released by eight of the leading progressive presidential candidates.
An obvious but important caveat: none of these audacious ideas will tap-dance its way into law or policy should its sponsor get elected. (The proto-autocrat decrees of our current incumbent might lull some into that assumption.) A new chief executive will need to inspire the House and Senate to a pitch of pro-active fervor not seen since the First Hundred Days of Franklin D. Roosevelt’s presidency when the New Deal took form in a blizzard of “relief, recovery, and reform.” For our present stumbling and divided Congress to suddenly sprout capes, masks, and flippers and get busy cleaning out the present rot may seem a stretch. Yet things can happen quickly, as the last midterms showed, and a whiff of activism does linger in the air.
With all this in mind, let us turn to the symbiotic manifesto that has arisen from those ordinary heroes at Ground Zero: “Grassroots 2020: A 5-Part Plan for Mental Illness SMI.”
Grassroots: 2020 has been personally distributed to visiting Democratic candidates or mailed to their offices by Leslie and Scott Carpenter of Council Bluffs, Iowa. The Carpenters’ tireless work has helped join the reformist trajectories of these politicians and the people.
I lay it out below with minimal editing, in summary form. You will note that each part of the plan delineates action that a president can undertake, sometimes independently of Congress. And unlike the candidates’ ideas above, Grassroots: 2020 addresses justice-reform issues (incarceration-trimming, for example) only incidentally. It focuses on existing rules, many of them arcane to the non-specialist, that nonetheless have caused decades of frustration and despair for those struggling to reclaim their afflicted loved ones from a decayed system:
A FIVE-PART PLAN TO ADDRESS SERIOUS MENTAL ILLNESS (SMI) 2020 PRESIDENTIAL CANDIDATES. PLEASE ADDRESS THESE TOPICS IN YOUR CAMPAIGN APPEARANCES AND DEBATES:
1. RECLASSIFY SERIOUS MENTAL ILLNESS (SMI) FROM A BEHAVIORAL CONDITION TO WHAT IT IS – A NEUROLOGICAL MEDICAL CONDITION
WHY RECLASSIFICATION IS IMPORTANT:
Re-classification will unlock more research funding and help eliminate discrimination in treatment, insurance reimbursement, and the perception of SMI as a “behavioral” condition. SMI is a human rights issue. The National Institutes of Mental Health ranks SMI among the top 15 causes of disability worldwide with an average lifespan reduction of 28 years.
PRESIDENTIAL ACTION:
• Create a cabinet position exclusively focused on SMI. • Push for Congressional appropriations to include schizophrenia in a CDC[efn_note]The federal Centers for Disease Control Institute[/efn_note] program that collects data on the prevalence and risk factors of neurological conditions in the U.S. population.
Overly strict HIPAA laws make it extremely difficult for families and caregivers to partner in the treatment of their loved ones, resulting in important life-saving medical information gaps. By eliminating this barrier, family support will be strengthened, reducing the chance of relapse, homelessness, imprisonment, and death.
PRESIDENTIAL ACTION:
Work with legislators to change HIPAA law to ensure mental health professionals are legally permitted to share and receive critical diagnostic criteria and treatment information with/from parents or caregivers of SMI.
3. REPEAL MEDICAID’S INSTITUTES FOR MENTAL DISEASE EXCLUSION (IMD).
WHY IMD REPEAL IS IMPORTANT:
The Medicaid IMD Exclusion prohibits Medicaid payments to states for those receiving psychiatric care in facilities with more than 16 beds for those in the 21-65 age group. This demographic represents the majority of SMI cases. Repeal of the IMD Exclusion will increase the availability of acute care, inpatient psychiatric beds. The IMD exclusion not only discriminates against those suffering from neurological brain disorders, it’s a leading cause of our national psychiatric hospital bed shortage.
PRESIDENTIAL ACTION:
• Work with legislators to repeal the IMD exclusion.
4. PROVIDE A FULL CONTINUUM OF CARE FOR THOSE WITH SMI
WHY A FULL CONTINUUM OF CARE IS IMPORTANT:
A continuum of care insures that SMI patients receive early intervention at all stages of their illnesses, long-term care when needed, and follow-up treatment (medications and therapies) when they’re released. Providing a continuum of care reduces: incarcerations, emergency rooms visits, homelessness, and death. A continuum of care provides life-time management that permits a patient to move without penalty from one level of care to another as needed.
PRESIDENTIAL ACTION:
• Create federal incentives to states which are addressing a full array of inpatient, outpatient, and supportive housing care.
5. DECRIMINALIZE SERIOUS MENTAL ILLNESS (SMI)
WHY DECRIMINALIZATION OF SMI IS IMPORTANT:
People suffering with other neurological conditions like Alzheimer’s and dementia can get treatment promptly without being kicked out of their homes to wander the streets until they are arrested and put in jail or prison rather than a hospital. Serious mental illness is the only disease where the doors to treatment are shut unless a crime is committed. This is pure and simple discrimination with the disastrous results we see in our country today — homelessness, incarceration, the disintegration of families, and death.
PRESIDENTIAL ACTION:
• Work with legislators to change “must be a danger to self or others” criteria. • Work with legislators to change involuntary commitment criteria, alleviating the subjective nature of “gravely disabled” and redefining it in objective terms based on scientific medical need for treatment. Psychosis, like a stroke, is a traumatic brain injury and needs immediate treatment for the best outcome.
Bernie Sanders
Returning to the candidates’ manifestos, I have omitted two demands that show up in most of them, yet are given no more than lip-service by none except Bernie Sanders: abolishing capital punishment and solitary confinement. Both are urgent. Deciding which is the most urgent depends, I guess, upon the morbid calculation of whether continued existence in the “hole,” with its barbaric history of destroying human personality, is worth the torture. I have felt my way to an agonizing decision. In my next blog I will urge the candidates to meditate on solitary confinement for exactly what it is, and to treat it as primary target for abolishment.
Well, not “no one.” Still, the levels of ignorance, too often coupled with hostility or sheer meanness, remain unacceptably high in this country. We in what I’ve called “the sub-nation” must never assume that the people we encounter will have even a working knowledge of severe mental illness: not a relative, a next-door neighbor, a caregiver, a police officer, a stranger in the park or on the street–not even the President of the United States.
Below are three recent bits of evidence that prove my point. The first is the text of a Facebook post by Scott Carpenter, a leading reform advocate based in Iowa.
Scott and his wife Leslie, who have seen a family member stricken, are among the strongest voices in America for what needs to be done. Yet not even they are immune from incidents of unexpected and bewildering hatefulness:
An elderly man walks [up to me] and says that ‘the problem isn’t about guns. It’s about crazy people.’
Leslie (against my advice to not engage) indicates that we have a son who has a serious mental illness and that he should come listen to he comments in an hour or so. He declined.
Then he said, ‘your son and all of the crazy people should be taken out in a field and shot. That way they could be useful as fertilizer’.
Please don’t ever think that a day of activism is easy.
Scott J. Carpenter”
When you have caught your breath from that, please follow the two links below.
The first link is to some remarks that President Trump made to campaign workers before a political rally in New Hampshire, in which he continues his strange and uninformed characterization of the mentally ill as, collectively, a horde of depraved killers that must be rounded up and swept into asylums. This and other tirades show that Trump knows nothing about insanity and cares less: his real agenda is deflecting attention from the ongoing mass-shooting crisis: The article leaves no doubt about this:
“Trump said many other Republican leaders and the public don’t want ‘insane people, dangerous people, bad people’ owning guns.”
“Words matter, Mr. President. ‘These people’ are our friends, neighbors, children, spouses. They’re not ‘monsters,’ ‘the mentally ill’ or ‘crazy people’ – they’re us. Talking about reinstitutionalization only further marginalizes and isolates the one in five people with mental illness. Instead, we need to be talking about the power of early treatment and effective intervention to change lives.”
These are but a couple of examples of incidents and attitudes that repeat themselves daily in America. They underscore the urgency of the seminal five-part manifesto organized by advocate Dede Ranahan and made widely available online and to presidential candidates last week. (Ranahan’s mentally ill son Patrick died in an institution in 2014.) The lessons in Ranahan’s great document are many and vital.
What I have outlined above constitutes just one. It is at once tiresomely repetitive and freshly urgent: We can never assume that any given individual–not even our Chief Executive–knows much about crazy people. And we must work relentlessly to change that.
P.S. Mental healthcare advocates Scott and Leslie Carpenter discussed the challenges they experienced when seeking proper care for their son Patrick during an interview withThe De Moines Register. What they share is both heartbreaking and informative. I encourage you to take a few moments to watch their interviews below to better understand how mental healthcare policies and procedures often fail to provide effective or compassionate care to the mentally ill. If you would like to share your own experiences of mental healthcare for yourself or a loved one, I invite you to comment below.
Stories from the front lines of Iowa’s mental health crisis
The documents below usher in a revolution. They describe a bold new movement, a national front organized to break the silence of the stricken and reverse the longstanding political neglect of America’s decrepit mental healthcare policies and institutions.
The advocate and author (Sooner Than Tomorrow) DeDe Ranahan has completed a wide-ranging national canvass of those in the “sub-nation”: the mothers, caretakers and advocates of people suffering from serious mental illness: schizophrenia, bipolar disorder, and related incurable afflictions.
DeDe Ranahan
Her tireless work has produced historic results: the first comprehensive, deeply informed list of things that absolutely need to be done to restore safety, humanity, and hope to a strata of victims that has been marginalized and abused since medieval times.
The dynamic advocacy team of Scott and Leslie Carpenter is distributing these documents to the candidates visiting Iowa prior to the Democratic presidential primaries. The Carpenters have reported that the response so far has been heartening.
DeDe Ranahan’s survey results are vital both in themselves and as building-blocks toward a future unification of efforts to reclaim the mentally ill and restore them to meaningful lives. She deserves the thanks of everyone who has been touched by this abhorrent malady. It seems that someone, after all and at long last, does care about crazy people.
SMI PLAN
TO: All 2020 Presidential Candidates
SUBJECT: Serious Mental Illness (SMI)
So far, 2020 political candidates make rare mention of serious mental illness (SMI — schizophrenia, schizo-affective disorder, OCD, bipolar disorder, and major depression), and the lack of mental illness care in the US.
* The SMI population represents 4-5% (10 million) of the mentally ill in the US. That’s 10 million families and extended families (voters).
* Ten times as many people with SMI are incarcerated as are hospitalized.
* Some SMI individuals are so sick they don’t realize they’re sick (anosognosia), don’t respond to treatment (if they get it) and end up incarcerated, homeless, missing, suicidal or dead.
It will cost billions to create a viable mental illness system. It’s costing billions, now, in prison over-population, homelessness and cities under siege, lost workdays, family disintegration, suicides, untimely deaths, inundated ER’s and hospitals, violence caused by untreated SMI, overwhelmed police, and in uninformed and misinformed criminal justice systems.
The Five-Part Plan enclosed is the collaborative work of grass-roots advocates from across the country —individuals, professionals, writers, journalists, caregivers, and mothers (always the mothers). Our intent is to put this plan in front of every 2020 presidential candidate. Right now, no candidate is talking about SMI. It’s as if it didn’t exist.
The steps in our plan are baby steps. We can’t immediately address everything that needs to be addressed in our messed up mental illness system, but we have to start somewhere. We’re trying to help 2020 candidates — we know you have a lot on your plates and we appreciate your energy and efforts to make our country better. We’ve created this Five-Part Plan to give you a starting point and a way to introduce SMI into political discourse and public conversation.
We’re asking you to take four initial actions:
1. Please read our plan and make it your own.
2. Put your SMI plan on your campaign website.
3. Talk about SMI on the campaign trail and in campaign debates.
4. Talk with members of the SMI community. We’re willing and able to help you as you move forward.
The SMI community is searching for its 2020 presidential candidate. We’re a large, passionate, motivated, frustrated, hurting, and determined block of voters. We look forward to hearing from you.
ENDORSEMENTS
Marie Abbott — Waterford, Michigan,
“My grandson has autism, bipolar disorder, and development delays. Has his civil rights intact.”
Jane Anderson — Illinois
“My 38 year-old son has paranoid schizophrenia. He was diagnosed at 18. My husband and I are caregivers.”
Tim Ash — Arcata, California
“Caretaker of a volatile, unstable SMI family member because there are no options besides jail and the bushes or doorways.”
David Bain — Sacramento, California
“I’m living with chronic depression and epilepsy and working to divert SMI from prison into treatment.”
Marti Rhoden Bessler — Alexandria, Kentucky
“My son’s been suffering from schizoaffective disorder for 19 years within our failed mental health system.”
Alisa Bernard — Jupiter, Florida
Judy Bracken — San Ramon California
“My 30-year-old son has schizoaffective disorder.”
Katherine Smith-Brooks and Bob Brooks — Carlsbad, California
“Our SMI son is now stable and working following effective treatment and the same psychiatrist for 20 years. We were his only advocates for many years.”
Regina Gipson Burns — Hoover, Alabama
Leslie and Scott J. Carpenter — Iowa City, Iowa
“Our son’s been suffering from under-treated schizoaffective disorder for 12 years. He lives in a group home with too few services. He’s been hospitalized 20 times.”
Mark Rippee
Sue Chantry — Vacaville, California
“I’ve lived here for many years and watched Mark Rippee, SMI and blind, on the streets of Vacaville with no mental health services.”
Barb Cobb — Iowa
“My SMI daughter’s been under-treated and under-supported by the current system. She’s endured over 20 hospitalizations and is barely surviving.”
Christine Cushing — Vacaville, California
“There are no resources or places to live for those who suffer from SMI. For a country that’s so progressed, we’re so far behind taking care of those with SMI.”
Lori Daubenspeck — St. Croix, US Virgin Islands
“My SMI son is a US Army vet. There’s no SMI facility here and one psychiatrist for the island. We’re in desperate need of facilities, doctors, and federal action.”
Kathy Day — Folsom, California
“My godson’s been discharged from hospitals many times while considered to be gravely disabled. Laws need to be based on need for treatment rather than time.”
Katherine Flannery Dering — Bedford, New York
“My brother, Paul, suffered with schizophrenia for 32 years of dwindling care. He died at age 48. “
Lois Earley — Phoenix, Arizona
“I’m the mother and legal guardian of an adult SMI daughter. I’ve been battling the behavioral health care system in Arizona since 2004.”
Darla Eaves — Everett, Washington
“My husband committed suicide. My son died in our psychiatric hospital. My daughter, thank God, is here with me and stays on her medication.”
Donna Erickson — Abington, Massachusetts
“My 34-year-old son has bipolar disorder. He’s been hospitalized 25+ times and cheated out of the life he wanted through no fault of his own.”
Sonia Fletcher —- Mount Shasta, California
“My daughter’s SMI was untreated when she shot and killed her father in a psychotic break. Our family is heartbroken and literally broken apart.”
Anne and Tim Francisco — Orange County, California
“Our SMI son was sentenced to prison for a nonviolent offense while he was in a state hospital. He ended his life by suicide while in solitary confinement.”
Lynne Gibb — Ojai, California
“My daughter’s suffered with schizo-affective disorder for 20 years. She’s been missing, homeless, and hospitalized, but never out of her family’s hearts and thoughts.”
Elaine D. Gilliam — Myrtle Beach, South Carolina
“My eldest son has paranoid schizophrenia. My eldest daughter committed suicide. Two children are wonderful retired military families.”
Linda (Rippee) and Joseph Privatte Lou Rippee – Vacaville California
“SMI blind son, brother, and brother-in-law. No mental health services for 3 decades. Solano County refuses to conserve.”
Betty Plowman
“I was a neighbor who observed this tragedy for 32 years and tried to help when no one else would.”
Chris Plowman
“I’ve watched this man waste away on the streets for 30 years untreated. Some people need our help and tax dollars; not be abandoned to rot. “
Pam Wilcoxson
“Mark’s family’s been fighting for help for him for many years and still have not gotten anywhere.”
Mark and Laura Harreld — Strawberry Point, Iowa
“Our SMI son was caught in the criminal justice system for non-violent crimes. He ended his life, to avoid another prison sentence, while in a hospital under armed guard.”
Dianne Harris — Grove City, Ohio
“My son died of a co-occuring vascular condition before a treatment was found for his negative symptoms of schizoaffective disorder. More research is needed desperately.”
Janet Hays — New Orleans, Louisiana
“I created Healing Minds NOLA to bring residents, families and stakeholders together to explore alternatives to incarceration, homelessness and death for those suffering with SMI.”
Amy Kerr and Paul Cox —- Pasadena, Maryland
“We’re caretakers for a 23-year-old son who has schizophrenia and a friend with major depression and end stage renal failure. “
Jeannie Kneisly-Manley — Elizabeth City, North Carolina
“My son has schizophrenia. He has a criminal charge and no court date to get him in the hospital. If I hadn’t bailed him out, he’d still be in jail waiting.”
Stacy Kollias — Henderson, Nevada
“I’m the mother/caregiver of a 30-year-old son suffering from schizoaffective disorder.”
Dianne Lam — Oakland, California
“My son has a dual diagnosis and schizoaffective disorder.”
Carole McAfee — Salem, Oregon
“My son is living with schizophrenia.”
Sherri McGimsey — Morganton, North Carolina
“My son is a Marine Veteran with schizoaffective disorder.”
Gerri Mele — Cleveland, Ohio
Linda L. Mimms, MA, — Poway, California
“The inability to get our ill family member prompt treatment has led to a worsened condition and uncertain prognosis which was totally avoidable.”
Alison Monroe — Oakland, California
“My 24-year-old daughter is a meth user who has schizophrenia. I’ve tried everything to keep her alive and off the street, with some success.”
Nancy Moody — Cambridge, Ohio
“My son has schizoaffective disorder. He’s suffering from withdrawal, seizures, tremors, cognitive impairment, and hallucinations. No one wants to help him.”
“My son has bipolar-schizoaffective disorder. While homeless, voices told him to hurt someone. He’s incarcerated while waiting for a bed in Napa State Hospital.”
Kelly Nidey — Vincennes, Indiana
“My son has struggled with bipolar/schizoaffective disorder for almost 15 years.”
Teresa Pasquini — Contra Costa County, California
“I’m mom to Danny who is surviving 20 years of suffering, suicidality, solitary, and schizoaffective disorder. There’s no federal action plan for families like mine.”
Darlene Patrick —Farmington, Maine
“My 32-year-old son has paranoid schizophrenia. He’s been in jail, the hospital, release, repeat.”
Gema Pena — Hialeah, Florida
“My son, Kristopher, was in solitary for 10 years. He attempted suicide, ate his own feces, was catatonic, and lost over 100 pounds.”
“I’m the father of two sons afflicted with schizophrenia. One took his life in 2005.”
Paula and Bruce Quertermous — Clinton Township, Michigan
“Our 39-year-old daughter has bipolar disorder and cognitive disability from birth.”
DeDe Ranahan with her son.
Dede Ranahan — Lincoln, California
Author: Sooner Than Tomorrow—A Mother’s Diary About Mental Illness, Family, and Everyday Life (2019). soonerthantomorrow.com. “My son died in a hospital psych ward in 2014. “
Margaret Reece and Greg Gazda — Butte County, California
“Our SMI son has been hospitalized 5 times, arrested, and is currently in a mental health court program and living in Yolo County with his grandparents.”
Arlene Renslow — Modesto, California
“I have two sons with brain damage. One son has schizophrenia. Unless someone does something, things will get worse for everyone.”
Mary (Courtney) Sheldon — Poway, California
“Mother of 24-year-old SMI son. We’ve winged it for 5 years. My SMI brother died, with his ‘civil rights intact’ behind a dumpster in Anaheim, California.”
Martha Mccollister Sroka — Dunkirk, New York
“My son has schizophrenia. It’s horrible watching your child change, struggle, and suffer. I request that SMI get the same attention and resources as any other medical illness.”
Joanne Strunk — Lexington, Kentucky
“My daughter’s been raped, homeless, hospitalized (40+times), and almost died lost in the woods for weeks. She’s dying of neglect due to SMI.”
Shelly and Scott Switzer — Sandpoint, Idaho
“We’re parents of a 33-year-old son with inadequately treated schizoaffective disorder in Missoula, Montana. SOS We’re barely hanging on.”
Diana Mandrell Troup — Texas
“My daughter spent 16 years in delusion and psychosis because of bad mental health care. She suffered 50+ involuntary holds, multiple tazings, and traumas.”
Laurie Turley — Maine
“My sister died due to HIPAA restrictions. One of the last things she said to me was, ‘They should have let you help me. I wasn’t in my right mind.’”
Monica and Kimmo Virtaneva — Hamilton, Montana
“Our son, Mika, took his life after the disease schizophrenia took his brain and the criminal justice system took his dignity.”
Cheryle Vitelli — Newark, Delaware
“I lived with my SMI son for 6 years while he was dangerous with only he and I in the house. Finally, a compassionate police officer pushed to get him help.”
Darlene Been Watkins — Moulton, Alabama
“My son, Shane, was denied treatment, while in psychosis, because there weren’t enough beds. Two days later, he was shot by police while I watched.”
Anna Wellnitz — Oro Valley, Arizona
“I’m diagnosed with SMI.”
FIVE-PART PLAN TO ADDRESS SERIOUS MENTAL ILLNESS (SMI)
FOR ALL 2020 PRESIDENTIAL CANDIDATES
PLEASE ADDRESS THESE TOPICS IN YOUR CAMPAIGN APPEARANCES AND DEBATES
1. RECLASSIFY SERIOUS MENTAL ILLNESS (SMI)) FROM A BEHAVIORAL CONDITION TO WHAT IT IS, A NEUROLOGICAL MEDICAL CONDITION WHY RECLASSIFICATION IS IMPORTANT Reclassification will unlock more research funding and help eliminate discrimination in treatment, insurance reimbursement, and the perception of SMI as “behavioral” condition. SMI is a human rights issue. NIMH ranks SMI among the top 15 causes of disability worldwide with an average lifespan reduction of 28 years. PRESIDENTIAL ACTION * Create a cabinet position exclusively focused on SMI. * Push for Congressional appropriations to include schizophrenia in a CDC program that collects data on the prevalence and risk factors of neurological conditions in the US population.
2. REFORM THE HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPPA) WHY HIPAA REFORM IS IMPORTANT Overly strict HIPAA laws make it extremely difficult for families and caregivers to partner in the treatment of their loved ones, resulting in important life-saving medical information gaps. By eliminating this barrier, family support will be strengthened, reducing the chance of relapse, homelessness, imprisonment, and death. PRESIDENTIAL ACTION * Work with legislators to change HIPAA law to ensure mental health professionals are legally permitted to share and receive critical diagnostic criteria and treatment information with/from parents or caregivers of SMI.
3. REPEAL MEDICAID’S INSTITUTES FOR MENTAL DISEASE EXCLUSION (IMD) WHY IMD REPEAL IS IMPORTANT IMD repeal will increase the availability of psychiatric inpatient beds. The IMD exclusion is not only discriminatory of those suffering from neurological brain disorders, it is a leading cause of our national psychiatric hospital bed shortage. It prohibits Medicaid payments to states for those receiving psychiatric care in a facility with more than 16 beds who are 21-65, the age group with the most SMI. PRESIDENTIAL ACTION * Work with legislators to repeal the IMD exclusion.
4. PROVIDE A FULL CONTINUUM OF CARE WHY A FULL CONTINUUM OF CARE IS IMPORTANT A continuum of care insures that SMI patients receive early intervention at all stages of their illnesses, long- term care when needed, and follow-up treatment (medications and therapies) when they’re released. It reduces visits to jails, ER’s and hospitals, homelessness, and morgues. A continuum of care provides life-time management. PRESIDENTIAL ACTION * Create federal incentives to states which are addressing a full array of inpatient, outpatient, and supportive housing care.
5. DECRIMINALIZE SERIOUS MENTAL ILLNESS (SMI) WHY DECRIMINALIZATION OF SMI IS IMPORTANT People suffering with other neurological conditions like Alzheimer’s and dementia can get treatment promptly without being kicked out of their homes to wander the streets until they are arrested and put in jail or prison rather than a hospital. Serious mental illness is the only disease where the doors to treatment are shut unless a crime is committed. This is pure and simple discrimination with the disastrous results we see in our country today — homelessness, incarceration, the disintegration of families, and death. PRESIDENTIAL ACTION * Work with legislators to change “must be a danger to self or others” criteria. * Work with legislators to change involuntary commitment criteria, alleviating the subjective nature of “gravely disabled” and redefining it in objective terms based on scientific medical need for treatment. Psychosis, like a stroke, is a traumatic brain injury and needs immediate treatment for the best outcome.
EXTENDED LIST OF SMI NEEDS
This list represents brainstorming ideas of advocates from across the country. They’re individuals, families, and professionals who are living/working with SMI. They have in-the-trenches experience. The list presents a partial picture of the depth and breadth of SMI issues that need to be addressed.
1. RECLASSIFY SERIOUS MENTAL ILLNESS (SMI) FROM A BEHAVIORAL CONDITION TO WHAT IT IS, A NEUROLOGICAL MEDICAL CONDITION.
2.REFORM THE HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT (HIPAA)
Present patients and families with a social worker to support the family unit throughout the care process, including medication and psychiatric treatment.
Require mandatory HIPAA training for everyone in the medical profession and mandate a test on proven knowledge.
Develop a federal program for the administration of an advance directive (PAD) which includes a universal release of information and designates an agent if a patient’s capacity is lost.
3. REPEAL MEDICAID’S INSTITUTES FOR MENTAL DISEASE EXCLUSION (IMD)
4. PROVIDE A FULL CONTINUUM OF CARE
Provide inpatient care (IMD waivers), outpatient care (i.e., AOT, Clubhouses), and housing ( a full array from locked stabilization to unlocked intensive, medium intensive, peer run, PSH, asylum).
Require a psychiatric standard of care for various SMI diagnoses like other medical specialties.
Require prescriptions based on need not ROI for the insurance industry
Remove ER’s as entry for mental illness hospitalization. The ER process and its chaotic environment aren’t conducive to the well-being of SMI patients.
5.DECRIMINALIZE SERIOUS MENTAL ILLNESS
Eliminate solitary confinement in jails and prisons.
Support nationwide civil mental health courts and expand criminal ones that are already established to keep SMI out of jails and prisons.
Establish mental health courts on a federal level, and coordinate federal courts and state-run mental illness facilities.
Move crimes that SMI commit in the federal system into state courts.
Mandate a way for families to provide medical history to jail/prison doctors to inform treatment.
Fund a digitized system for medical records in counties/hospitals to jails so information can be transferred immediately upon arrest and incarceration.
Provide uniform psychiatric screening of the incarcerated.
Use standardized protocols for medication of SMI prisoners.
Require strict limits on waiting for trial time.
6. PAY ATTENTION TO SUPPORTIVE HOUSING
Provide 24/7 supervised housing for those who cannot live independently.
Provide defined levels of support built around a person’s needs, especially long-term care.
Clarify Olmstead for SMI. Lease restrictive care isn’t always least expensive or best.
Examine, don’t ignore, a person’s ability to handle and benefit from a less restrictive setting.
7. REVAMP INVOLUNTARY TREATMENT
* Use lack of insight (anosognosia) and grave disability as criteria for determining involuntary treatment.
Establish a federal standardized “need for treatment” involuntary commitment law.
Base restrictive settings on actual abilities, not wishful thinking or one-track plans.
8. INCLUDE EDUCATION
Require mandatory, institutionalized education about SMI for judges, sheriffs, attorneys, district attorneys, law enforcement, and first responders.
Require units of SMI education for educators — preschool through university.
Revamp Crisis Intervention Training and expand training to all counties.
Provide a health proxy form for college students to allow them to release medical information and name who can take care of them in a crisis.
Hold universities accountable and required to connect students to crisis intervention, especially during medical leave.
9. GIVE INCENTIVES
Incentivize the expansion of medical schools to graduate more psychiatrists, child psychiatrists, internists with psychiatry specialties, psychiatric nurse practitioners and physician assistants.
Allow loan forgiveness for providers treating SMI.
Give incentives for rural psychiatrists.
Incentivize more long-term treatment/stabilization of SMI.
Give incentives to psychiatrists to accept health insurance, especially Medicaid.
10. EXPAND ASSISTED OUT-PATIENT TREATMENT (AOT)
Federally clarify AOT and create a federal model for AOT law
Offer AOT immediately to everyone upon diagnosis.
11. IMPROVE HOSPITALS
Build regional federal hospital for patients who cannot be treated in their home state’s hospitals because of lack of beds.
Improve reimbursements to hospitals which lose revenue on SMI patients.
End hospital discrimination against SMI “violent” patients and those “difficult to discharge.”
12. INCREASE RESEARCH AND EPIDEMIOLOGY
Fund NIMH research specifically for SMI.
Establish a Disability Advocacy Program for legal services for SMI when counties/states fail to provide long-term support services or when insurance/managed care and Medicaid fail to cover/pay for long-term supported services and treatment.
Pursue better national epidemiology studies for people with SMI.
Establish a federal law that requires states to track each SMI diagnosis with bad outcomes like death, homelessness, and incarceration.
13. REVISIT PARITY
Clarify parity for SMI and include Medicaid and Medicare in parity law.
Enforce violations against parity law.
14. ADDRESS SOCIAL SECURITY AND DISABILITY INCOME ISSUES
Change the way social security income for the disabled is taken by states when a patient is admitted to state operated mental health institutions, residential care facilities, and hospitals.
Increase disability income to a level where a person can survive and maintain reasonable housing.
16. CREATE PSYCHIATRIC CAMPUSES
Build psychiatric campuses with multiple levels of care, supportive housing from most restrictive to least restrictive, and separate independent living apartments.
Provide on-campus coffee shops, gyms, recreational facilities, and gardens where people with SMI could work with support as needed.
Provide substance abuse treatment services, AA or NA meetings.
In the aftermath of two traumatic mass shootings, the president re-invokes a horrid, distorted falsehood about the mentally ill.
And there it is: history’s defining damnation of sufferers of incurable damage to the brain, distilled into a three-word phrase of transcendent ugliness and stunted understanding.
The phrase was uttered on Monday. It was uttered to identify the provenance of the weekend’s massacres by shooters using legally purchased high-capacity semi-automatic weapons toward their collective harvest of 31 people dead and some 50 wounded.
The phrase was uttered by the President of the United States. It left stains, stains which, in moral and intellectual terms, replicated the stains of blood shed by the shooters’ victims.
Donald Trump | Image Credit Gage Skidmore via Flickr
Blaming “mentally ill monsters” (or “nut jobs,” or “wackos,” or “lunatics”) for such carnage is a morally repugnant, if time-tested device for shifting the public’s passion for safety away from gun control and toward the presumed demons in our midst. The president could not have been more transparent in exploiting the device. “Mental illness and hatred pulls [sic] the trigger, not the gun,” he instructed us, going on to label one of the shooters as “another twisted monster.”
In fact, it is a settled truth in psychiatric research that victims of brain afflictions are no more prone to violence than the general population. The prominent advocate Dj Jaffe makes an important stipulation: that the untreated mentally ill—those not stabilized by antipsychotic medications—can be more likely to cause harm to themselves or others. Still, implying that mental illness itself equates to degenerate aggression serves only to further isolate and punish the most helpless members of our society; to herd them back toward the dark corners and confinements of “insane asylum” days.
And herein lies the “intellectual” stain that President Trump’s words help spread: most people—like the president himself—do not understand mental illness: what it means, how it occurs, how it differentiates, why its victims behave as they do, and how even its most abject sufferers can be aided, often stabilized, by medications and therapy. In this vacuum of understanding, people tend to substitute prejudice, false science, myth, and hostility toward “crazy people.”
Briefly:
“Serious” mental illness—the kind in question here—is rare and unique. And incurable. Unlike alcoholism or anger or depression, serious mental illness is rooted in genetic flaws of the brain. Its various names include schizophrenia, schizoaffective disorder, bipolar disorder—similar yet not interchangeable conditions. It results in a loss of reason and rational control; hallucinations and the hearing of voices; alienation from family and friends; and, yes, sometimes—rarely—violence.
My wife and I have educated ourselves about serious mental illness because we’ve had to. It invaded our family several years ago, causing the suicide of a beloved son. Unfortunately, this is the painful route to understanding for most people: a loved one is stricken.
The costs of this cluelessness describe a cone of destruction that widens from the stricken individual through society.
The cone draws in and ravages parents and siblings of the stricken. It can cripple the finances of families without adequate insurance to cover treatment and medications. It drains human capital from the workforce, and thus economic revenue. It reduces the budgets of hospitals that can’t get reimbursement for their mentally ill patients. It overburdens police, whose lack of training and, sometimes, self-restraint, can result in death by gunshot of unarmed people in psychosis. It coarsens our criminal-justice system: think of schizophrenic adolescents hustled into jail by untrained or uncaring judges, where they await trial—often for weeks and months—while their unmedicated psychosis deepens. Think of solitary confinement. Think of a brain-afflicted child, perhaps your own (as countless parents must) ensorcelled in a cell, abused by fellow inmates and guards, with no end in sight, no comprehension. No hope.
Now think about “mentally ill monsters.”
Mentally ill monsters are not the source of our current crisis of public massacres. The monster is the gun: too many guns, with too little restraint and oversight regarding purchase. To his credit, President Trump gave lip service to keeping guns away from those “who pose a grave risk to public safety,” and to strengthening gun laws generally.
But leave the gun issue aside. Part of any president’s duty—a foundation of his “bully pulpit”—is to educate his fellow citizens on matters of complexity and urgent public import. The nature of serious mental illness, and the reclamation of its victims, comprise one such matter. The president could make a great, galvanizing contribution to ending the centuries-old oppression of “crazy people.” He could lead us in that direction. He could educate us. But first he must educate himself.
QUINCY — After Ron Powers’ youngest son committed suicide in 2005, the Pulitzer Prize winner and prolific author swore that he would never write about the “hellish” pain that he and his family went through.
“I was in a daze in the first five years, then the healing began, and I realized after reading more about the disease (schizophrenia) that I really had to do this,” Powers said.
Powers’ book starts with the words: “This is the book I promised myself I would never write.” But as he began going back through photos, emails and other items that belonged to his youngest son, Kevin, Powers saw the need to tell the world that ignoring mental illness is a terrible mistake and a social injustice.
National statistics indicate that more than 10 million Americans will suffer a serious mental illness each year and with more than three people in the average home, more than 34 million American lives will be disrupted.
Powers’ older son, Dean, was diagnosed with schizophrenia only months after Kevin’s suicide. Thanks to informed treatment choices, Dean’s illness has been controlled.
But too many people with mental illnesses are sent to jails, Powers said.
“The moral necessity for us as individuals, and for our country, is to reclaim these people,” Powers said.
“There’s primal fear and prejudice against the mentally ill and because of that, (society) punishes the mentally ill when we should be treating them.”
Since his book was published, Powers has been scolding the government for spending $31,000 per year to jail the average person with mental illness, rather than spending the $10,000 needed for treatment. He also has promoted programs that help those with mental challenges.
“Organizations around the country, like Transitions, are taking up the slack, and I’m so gratified that people are doing what they can to help,” Powers said.
Barb Baker Chapin, director of development at Transitions, hopes that Powers’ visit will help people see mental illness in a new light.
“One in five of us will suffer from a mental illness at some time in our lives, and yet there’s still such a stigma associated with it,” she said. “I hope Ron Powers’ very personal story can help us have a dialogue about the changes we need to see in the mental health system and the way we’re funding it.”
Powers has written 16 books, including “White Town Drowsing,” which looked at his hometown of Hannibal during the 1980s. He also wrote a biography of Mark Twain, “Mark Twain: A Life” that was a New York Times best-seller and a finalist for the 2005 National Book Critics Circle Award. In more recent years, Powers was co-author of “Flags of Our Fathers” and “True Compass,” which were both No. 1 New York Times hard-cover nonfiction best-sellers.
He was awarded the Pulitzer Prize for his critical writing about television for the Chicago Sun-Times in 1972. He also won an Emmy Award in 1985 for his commentaries on “CBS News Sunday Morning with Charles Kuralt.”
Several of Powers’ books will be available for sale. A complementary copy of “Flags of Our Fathers” will be presented to those who buy tickets to a social hour with the author, and he will do a book signing.
Ticket information for “An Evening with Pulitzer Prize-Winning Author Ron Powers on April 26
Meet and greet tickets are $75 for the 6:30 p.m. social hour, complementary copy of ‘Flags of Our Fathers,’ the chance to meet Powers during a book signing and preferred seating.
Preferred seating tickets are $25 each.
General admission tickets are $15, with doors opening at 7:30 p.m.
Tickets are on sale at the Oakley-Lindsay Center box office at 217-222-3209, or online at http://www.1qct.org/.
As the father of two sons with schizophrenia, author Ron Powers is familiar with the pain and frustration of dealing with a chronic, incurable disease of the brain.
Powers’ younger son, Kevin, was a talented musician whose struggles with schizophrenia began at age 17. Just before his 21st birthday, in 2005, Kevin took his own life.
A few years later, Powers’ older son, Dean, started experiencing symptoms of schizophrenia and had a psychotic break.
Ron Powers, a Pulitzer Prize-winning journalist and media critic, wrote Flags of our Fathers, which was adapted into a film by Clint Eastwood.Sarah Junek/Hachette Books
“There is no greater … feeling of helplessness than to watch two beloved sons deteriorate before [your] eyes, not knowing what to do to bring them back,” Powers tells Fresh Air‘s Terry Gross.
Powers’ new book, No One Cares About Crazy People, is both a memoir about his sons and a history of how the mentally ill have been treated medically, legally and socially. Although Dean is now medicated and doing well, Powers notes that many people with schizophrenia don’t receive the treatment they need — in part because they often don’t believe they are ill.
“This unwillingness to believe that one is afflicted has led to tremendous problems,” Powers says. “To force that person into being helped is a violation of his or her civil rights … and the law may penalize the care workers who give [people with schizophrenia] medications or admit them to a hospital against their will. … That is the great reigning Catch-22 of the way our society deals — or fails to deal — with schizophrenia.”
Interview Highlights
On why symptoms of schizophrenia often surface around the age of 17
It has to do with the maturation of the brain. … In order to start functioning as an adult brain, the brain must undergo a period of what is called “synaptic pruning,” really a cleansing away of all of the neurons, all of the connective material that is built up since infancy. That is no longer useful and it’s quickly replaced, but there is a period of vacancy, almost, in which the brain is very vulnerable to any kind of disruption. It’s unprotected, and this is the period of life, roughly clustered around the age of 17, when the disease can make its appearance.
On how denial impacted his sons’ treatment
Each of our sons was afflicted with this companion condition called anosognosia. … [It’s] defined as an inability to understand the self, a blockage of insight into what is happening. Many, perhaps most, of schizophrenic victims deny that they are schizophrenic, and this has led to many important social and legal and ideological conflicts. … The denial that took place, with Kevin the symptoms occurred before he reached the age of 18, meaning he could be treated without his consent. He was a juvenile and he was taken into care and custody without his consent.
Dean was over the age [of consent] and resisted treatment, denied that he needed to be treated, and it was only after a series of psychotic breaks that he came around to the understanding that he needed help.
Dean is accountable to a clinician. He has to report; there is a record of him taking his meds. Kevin was taking oral medication only on his own consent and we weren’t sophisticated enough to perceive that instead of taking the meds Kevin might be hiding the meds. This happened in the later stages of his descent and it was after he finally announced to us, “I’m fine. I’m healed. I’m OK, I’m not going to take my pills.”
Within a few months after that, Kevin hanged himself in our basement.
On trying to understand the degree of Kevin’s suffering
He was hearing voices. We know that. We could watch him through the kitchen window as he walked out of the house and toward the hot tub that he loved to sit in. We could see him climb into the hot tub and sit down, his profile was to us, and we could see him laugh. He would laugh, he would giggle. … Something was talking to him, and I think because of that happy response we saw from him we told ourselves that he had made friends with the voices, that the voices were beckoning him, they were coaxing him into their world, and that he finally decided to join them. I don’t know whether that’s true or not. I’ll tell you that it got me through the first five years of trying to figure out where Kevin’s mind had gone.
On still having dreams of Kevin
In the dreams Kevin is alive. He’s a small boy, around 10, 11, 12 years old. We know he’s a gifted guitar player, but he’s stopped playing his guitar, and he won’t start again. The odd thing is that both Honoree and I have had this dream. It might be a metaphor for his death, but he shows up, almost every night, as I say. … I’m glad to see him. In the dreams he is etched so perfectly. The reality of him, the physical sharp-focused reality of Kevin is overwhelming and all of his kindness and his goodness are there.
The advent of the so-called “wonder drugs” like Thorazine … were touted as cures for schizophrenia — they weren’t. At best they were cures for symptoms. But on the strength of Thorazine and its great consumer success and promise, President Kennedy, seeking to do the right thing, signed legislation … in 1963 … that authorized the emptying out of mental asylums and the transferring of their patients, their inmates, hopefully into community care centers that were going to be built around the country to receive them.
Deinstitutionalization was a catastrophic social experiment, one of the worst we’ve ever had. It ended up creating the [mentally ill] homeless population that still plagues us today.
The second terrible effect of deinstitutionalization was that many of the people never ended up in the community centers. The government ran out of money. They couldn’t build enough to contain this outflow of patients, so they ended up on the streets, and from the streets they ended up in prison. Many of them. Today our prisons are overflowing with the mentally ill. Prisons are our de facto mental hospitals.
The pitfalls and perils of marijuana legalization are well-documented. But whenever we discuss that research here on BreakPoint, we’re accused of not having the right research. What that means is that we’ve used studies that contradict the very vocal advocates of weed.
Well, let’s see what happens when we cite The British journal The Lancet, which, along with the New England Journal of Medicine and the Journal of the American Medical Association, is considered the “gold standard” for peer-reviewed medical research. It doesn’t get more “real” than being published in The Lancet.
A just-published study in The Lancet involving, among others, researchers at King’s College London, compared 900 people who had been treated for psychosis with 1,200 people who had not. Sample participants were drawn from across Europe and Brazil.
By “high-potency” the researchers meant marijuana with a THC content of more than ten percent. To put that figure in context, a study of the weed seized by the DEA between 1995 and 2014 found the THC content went from about 4 percent in 1995 to 12 percent in 2014.
Today, it’s not uncommon to read of marijuana that’s legally-sold in places like Colorado with THC content above 20 percent, occasionally 30 percent! Legalization advocates minimize the exponential growth in potency by saying that twenty or more years ago, Americans didn’t have access to “the good stuff.”
Well, that misses the point by several astronomical units. The point is that those people who daily use “the good stuff” are five times more likely to find themselves in a hospital suffering from delusions and hallucinations, to name only two symptoms of psychosis.
Now, critics will respond, “That’s correlation, not causation.” And that’s the criticism leveled at journalist Alex Berenson, author of Tell Your Children: The Truth about Marijuana, Mental Illness and Violence, a book I recommend highly. But as I heard Berenson say just last week in Denver, of course it’s correlation and not causation. The only way to prove causation would be to ask half a sample group to experiment with something that may harm them. That’s not ethically possible. By the way, all the studies that made us believe that cigarette smoking causes lung cancer were correlated studies too, but that was enough to convince us all.
Even so, writer Ron Powers doesn’t need a peer-reviewed study to convince him of the link between marijuana use and psychosis. In his 2017 book, Nobody Cares About Crazy People, he tells the moving story of his two sons, Dean and Kevin, who were both diagnosed with schizophrenia in their late teens.
As Powers tells readers, while there is a strong genetic component to schizophrenia, there is no “schizophrenia gene.” Instead, it’s a constellation of genetic and environmental factors that make people susceptible to schizophrenia. One of these, as Powers painfully learned, is heavy marijuana use, especially in the teenage years.
Of course, some people will tell you that they and most people aren’t mentally ill, so there’s little if any risk. But for a host of reasons, no one can know that with certainty. In fact, all pronouncements about how safe marijuana legalization is simply overstates the case.
That’s exactly what happened here in Colorado. The possible pitfalls were denied or downplayed. And so, Colorado now holds the dubious distinction of leading the country in first-time drug use. And the rate of monthly marijuana use among 18-to-25-year-olds in states with legal weed is nearly three times as much as states that haven’t legalized it. By the way, 18-25 is the age when schizophrenia often begins to manifest.
Given the well-documented mental health risks, especially to not-fully-formed adolescent brains, the rush to legalization is the height of irresponsibility. An irresponsibility that can shatter lives. And don’t just take our word for it.
BreakPoint is a Christian worldview ministry that seeks to build and resource a movement of Christians committed to living and defending Christian worldview in all areas of life. Begun byChuck Colson in 1991 as a daily radio broadcast, BreakPoint provides a Christian perspective on today’s news and trends via radio, interactive media, and print. Today BreakPoint commentaries, co-hosted by Eric Metaxas and John Stonestreet, air daily on more than 1,200 outlets with an estimated weekly listening audience of eight million people. Feel free to contact us at BreakPoint.org where you can read and search answers to common questions.
John Stonestreet, the host of The Point, a daily national radio program, provides thought-provoking commentaries on current events and life issues from a biblical worldview. John holds degrees from Trinity Evangelical Divinity School (IL) and Bryan College (TN), and is the co-author of Making Sense of Your World: A Biblical Worldview.
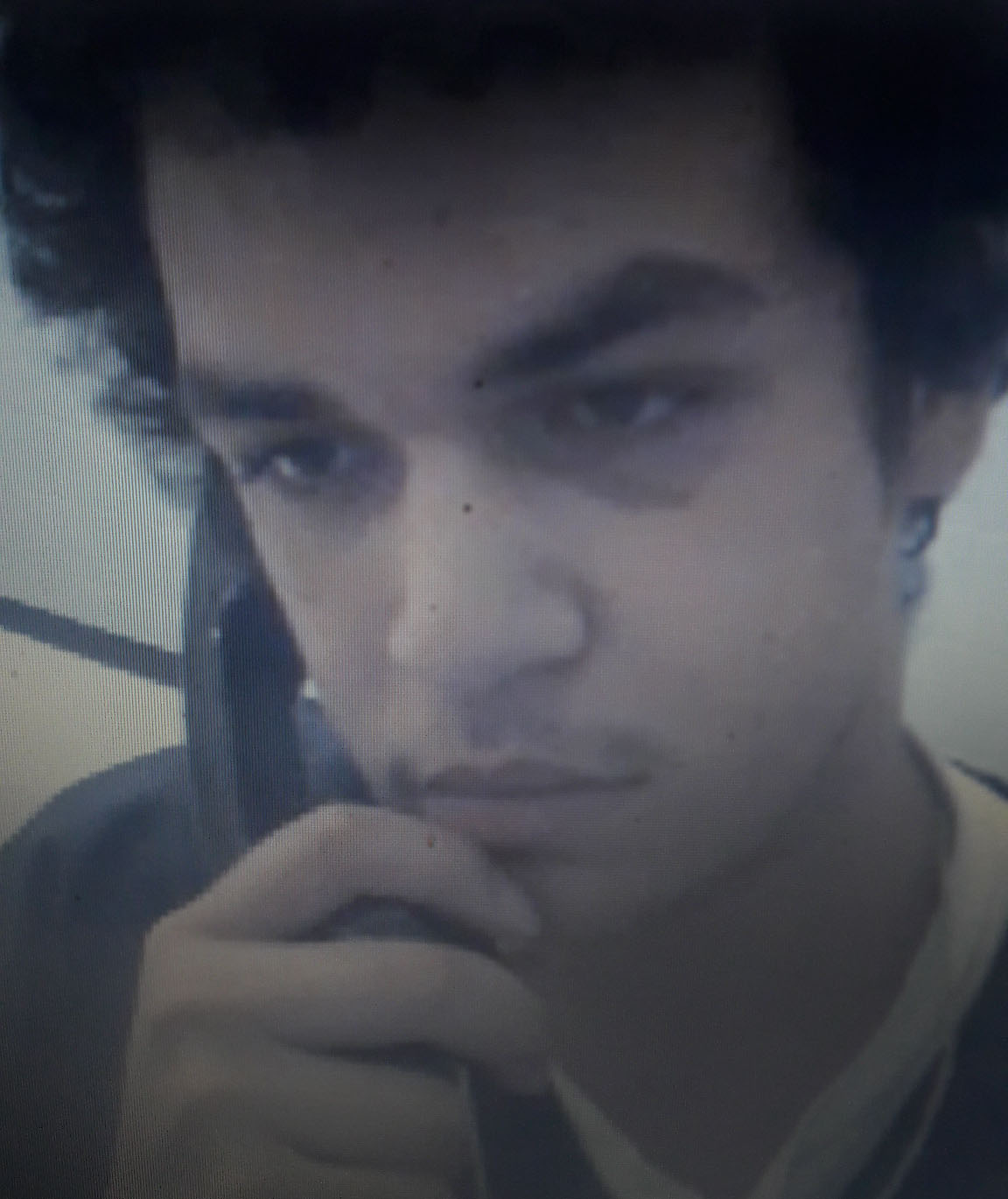
Tyler West is in a prisoner in the Richard Handlon Correctional Prison in Ionia, Michigan. Mark Rippee, blind and severely disabled, as well as severely mentally ill, is at large on the streets of Vacaville, California, where he has somehow survived for twelve years. He is regularly beaten up and tormented by street punks. His sister Linda Privette told me that in addition to food and clothing, she recently provided him with his eighth walking cane in a twelve-month period–the other seven had been taken from him.
Mark Rippee
You may read about Tyler and Mark, and the grossly inhumane reasons for their medieval persecution, elsewhere on this blog. In brief, each is an unconscionable victim of an American state’s official contempt for the mentally ill, contempt that festers from ignorance, indifference, and a lack of organized public pressure to rescue them and their families from their living hell.
I’m sure that many relatives of the mistreated mentally ill would like to see equal attention devoted to their loved ones. My inadequate response is that there are not enough megabytes in cyberspace to tell the story of every American sufferer of mental illness who has been further victimized by our systems. We need to make mental-health reform a massive civil-rights issue. We need a revolution of conscience.
Tyler West
I am posting below a heartbreaking, eloquent message from Tyler’s adoptive mother, Kimberlee Cooper-West. (She submitted it to the Facebook site Circle of Comfort and Assistance Community, and I reprint it with her permission, and it bears close reading.) You can find comments from Mark Rippee’s sisters, Linda Privette and CJ Hanson, elsewhere on this blog.
KIMBERLEE COOPER-WEST
Wish I had good news to share with ya all’ Love my CCA family! Some have asked, so here it is! Today is our son Tyler’s 20th birthday! We were unable to say Happy Birthday, as he is in lock down for 5 days. We drove a little over an hour, to Richard Handlon Correctional Prison, in Ionia, Michigan. This was last Monday. He is number #113697. We had cake with him. He made a cake from 2 honeybuns, smashed peanut M&Ms(sprinkles) and a melted Snickers bar on top. He is inventive. We sang Happy Birthday to him. He is still our boy! Few mention him. Our heart breaks for what, we have lost. This Will be his 3rd year, away, for his Birthday. Next he will miss Thanksgiving and Christmas. He hasn’t been given counseling, education, training, or the proper medications. He was beat up 4 times, since he was incarceration. Why, couldn’t these mental health professionals, keep him, in an, inpatient psychiatric hospital? For the love of God, there was no good reason, to release our son. His safety compromised. No one responsible. He was nearly shot at for trespassing. He was inpatient, 5 days prior, to his arrest.. He was delusional and hearing voices. What is wrong with this country? Why is there, no long term treatment? This is a brain disease, ya all’ Maybe we should start locking up every Grandma and Grandpa who is violent, or disorderly from Alzheimer’s. Serious mental illness a disease. It is prodromal to Alzheimer’s. Prisons are corporations. Their goal is money. They need prisoners. Caught up in the system, it is a real thingl. We are receiving, a criminal justice system education. Months are now years. One caseworker, Ms. Williams, calls many people names like dumb, retarded, idiots and pedophiles etc. Everyone in Ty’s facility is either mentally ill or autistic. She told Tyler a 19 year old kid, who was only supposed to be there for 2 months, your doing 15 years. It leaves me to wonder, how many, have given up from her words.. He is not even provided an inhaler for asthma, and chronic lung disease. He has autism and a serious mental illness. When he was in school he was never suspended. He was a target for bullies, which was, Our main concern. Incarceration, never crossed our minds. Today on his birthday, I sent his appeal papers, certified to a judge. Hopefully he will give him an apeallate lawyer.
This Arkansas group, #ARmindsMatter, looks to be a prototype for citizen-based activism in all our states to demand relief from the many failures in America’s systems of mental healthcare.
I would be interested to learn of similar movements in other states. With an active, agenda-driven interlinkage of groups such as #ARmindsMatter, we could forge a powerful watchdog, lobbying, and organizing collective that would establish reform as the civil rights issue of our time and break the inertia that’s destroying the lives of so many mental illness sufferers and their families.